Expression of a proliferation signature predicts sensitivity to genotoxic chemotherapy in oligometastatic colorectal cancer
Published in Cancer

The portal circulation facilitates early metastasis of colorectal cancer to the liver, which is fatal for most patients. However, a subset of patients with colorectal liver metastases present with limited spread of their disease, termed oligometastases, which are potentially curable with local therapies, such as surgical removal, radiotherapy, or radiofrequency ablation1. Improving survival for patients with colorectal liver oligometastases and identifying patients most likely to benefit from additional systemic therapy remains an important unmet need. Multiple randomized trials failed to demonstrate improved survival with the addition of cytotoxic chemotherapy to surgery2–4. Heterogeneity in tumoral features likely contributes to the differential outcomes and treatment sensitivity to cytotoxic chemotherapy in the setting of colorectal liver metastases. Therefore, further elucidation of potential mechanisms of chemoresistance may enable selection of patients most likely to benefit from adjuvant cytotoxic chemotherapy.
We previously identified three intrinsic molecular subtypes of mismatch repair proficient colorectal liver metastases designated as canonical, immune, and stromal subtypes1. Immune metastases exhibited favorable survival in the setting of immune infiltration alongside interferon and p53 pathway activation. By contrast, canonical metastases demonstrated adverse prognoses and overexpressed cell cycle and proliferation pathways in an immunologically cold tumor microenvironment. Despite their overall poor prognosis, a subset of patients with canonical metastases paradoxically exhibited favorable survival1.
In this context, we examined whether the molecular characteristics of the colorectal cancer liver metastasis subtypes were associated with differential benefit from the addition of chemotherapy to surgery. Across three robustly annotated clinical datasets (n=336) encompassing patients from two independent institutions and a randomized clinical trial, we found that elevated expression of a CIN70 gene expression signature5—which had previously been linked to cellular proliferation in the context of tumor aneuploidy—predicted adverse survival after controlling for known clinical and prognostic factors. High CIN70 colorectal liver metastases not only recurred more often but were also more likely to spread to multiple organ sites beyond the liver, which was often fatal for patients.
We wondered whether patients with low CIN70 colorectal liver metastases experienced better outcomes because their tumors were inherently more sensitive to DNA-damaging chemotherapies, such as topoisomerase inhibitors, which are routinely used in the treatment of colorectal cancer. Unexpectedly, we found the opposite to be true: high CIN70 tumors were more sensitive to topoisomerase inhibitors, but not chemotherapeutic agents which do not act through a mechanism of DNA damage.
Since high CIN70 tumors exhibited strong responses to genotoxic agents, we wondered whether DNA-damaging therapies depleted highly proliferative tumor cells resulting in improved clinical outcomes. To test this hypothesis, we examined four independent patient datasets with matched tumor samples before and after cytotoxic chemotherapy. We found that genotoxic chemotherapy typically decreased CIN70 scores; however, the magnitude of decrease was linked to response. Tumors that responded exhibited a larger decrease in CIN70 scores following treatment than those tumors that did not respond. We also found that tumors with low baseline CIN70 scores, indicating a less proliferative phenotype, experienced smaller decreases in CIN70 following therapy.
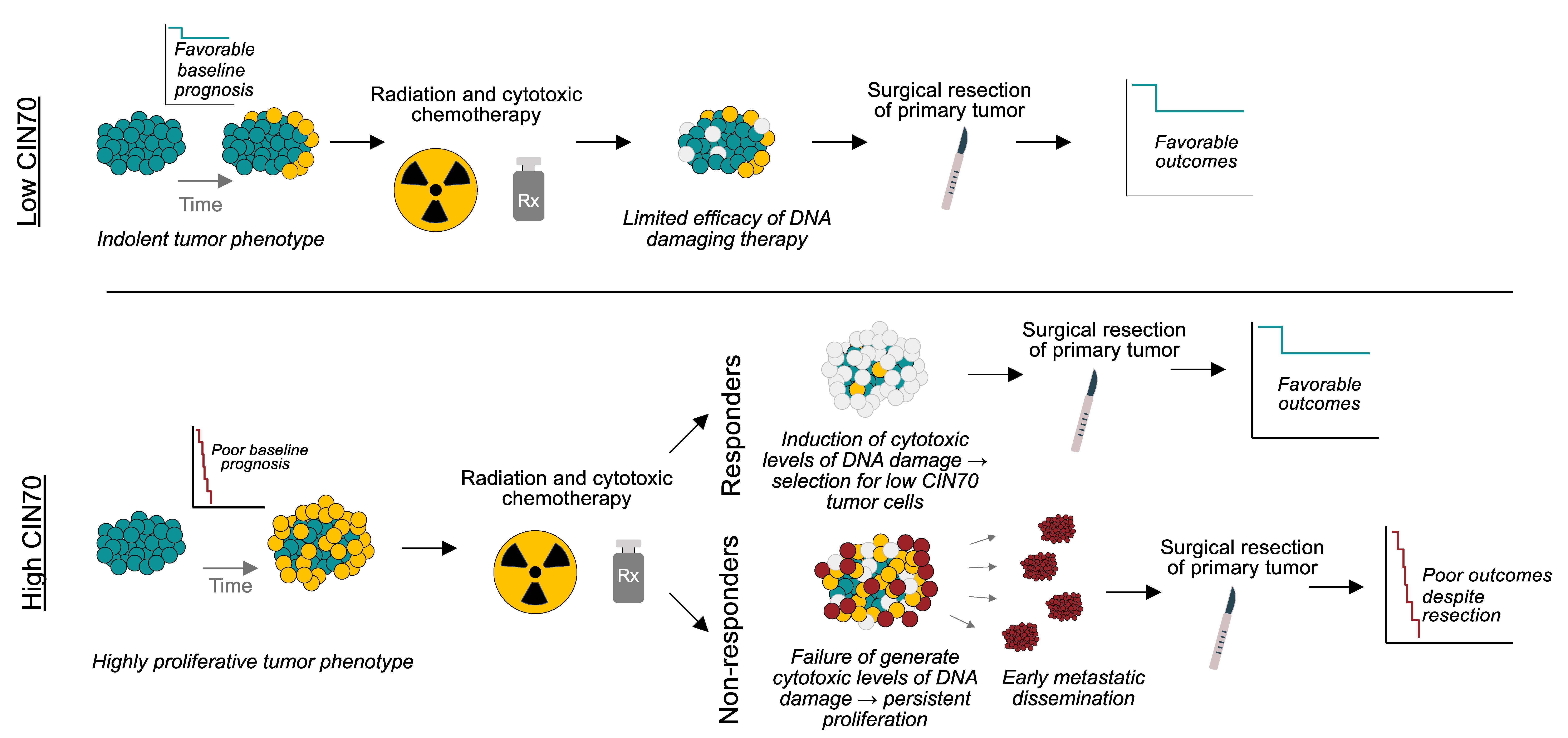
Taken together, we propose that low CIN70 tumors have a favorable baseline prognosis, despite exhibiting minimal responses to DNA damaging chemotherapy (Figure 1). By contrast, initially aggressive, highly proliferative (high CIN70) tumors have an unfavorable baseline prognosis which can be improved if CIN70 decreases in the response to DNA damaging chemotherapy. However, a subset of high CIN70 tumors harbor intrinsic resistance mechanisms rendering cytotoxic therapy ineffective, which leads to widespread metastatic dissemination and precludes successful disease control after tumor resection.
Our findings outline a strategy to personalize chemotherapy for patients with colorectal liver metastases. Building off our previously defined molecular subtypes, our study provides a next step towards improving treatment selection for patients with colorectal cancer liver metastases. Specifically, for patients whose tumors demonstrate aggressive biology (high CIN70), the benefits of improved disease control following genotoxic therapy likely outweigh the potential toxicities. On the other hand, patients with low CIN70 colorectal liver metastases are unlikely to benefit from chemotherapy and thus could be spared from the potential side effects of chemotherapy.
Nevertheless, these hypotheses should be tested in prospective trials. In addition, further studies are needed to understand the heterogeneity in response among high CIN70 tumors. Despite these limitations, we show that CIN70 holds promise as a complementary biomarker to previously defined molecular subtypes for assessment of prognosis and chemotherapy treatment selection. Beyond colorectal liver metastases, CIN70 might also be useful in personalizing treatment decisions in many human cancers, such as breast and lung cancer.
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Next-Generation AI in Drug Design for Precision Oncology
Publishing Model: Open Access
Deadline: Apr 01, 2027

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in