From Urban Planning to Respiratory Health: Why Weighting Risk Factors Matters 🏙️➡️🫁⚖️
Published in Earth & Environment, Plant Science, and Public Health

Whenever I attended conferences and academic seminars, public health impacts were explained differently each time through urban, environmental, or socioeconomic dimensions. Each discipline offered its own lens, its own framework.
But one question kept returning: 🔁❓
If respiratory diseases are the result of multiple interacting configurations urban, environmental, and socioeconomic how much weight should be assigned to each ? And why do we still struggle to translate scientific evidence into clear territorial priorities ? ⚖️📊
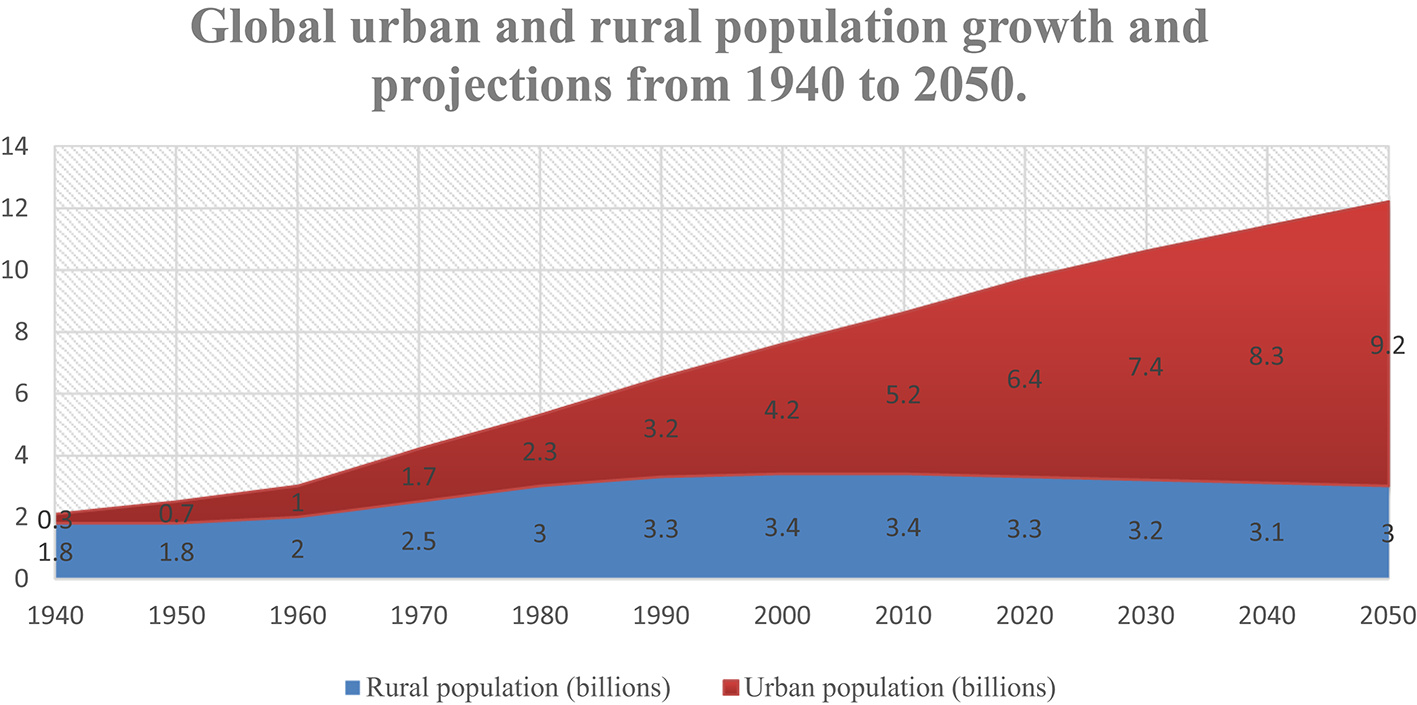
Cities are expanding rapidly. Pollution levels are rising. Climate change is reshaping exposure patterns. Social inequalities are deepening. And respiratory diseases from asthma and COPD to tuberculosis and COVID-19 continue to affect millions of people worldwide. We already know many individual risk factors: air pollution, housing overcrowding, traffic-related emissions, heat waves, lack of green spaces. The literature is abundant.
Yet something was missing.
What was lacking was a structured and transparent method to prioritize these factors to assign weight to each dimension and to validate findings through quantitative and econometric analysis, both for academic researchers and, especially, for policymakers who must decide where to intervene first.
It was precisely this gap that inspired the research titled “Environmental Urban and Socioeconomic Risk Factors for Respiratory Diseases: A Systematic Review with Quantitative Weighting Analysis.”
The Challenge of Fragmented Knowledge 🧩
We produce studies.
We accumulate data.
We publish analyses.
The literature in urban health is vast. Air pollution. Housing. Urban heat. Social inequalities. Daily mobility.
Each study adds a piece to the puzzle.
But the city is not a static puzzle.
It breathes. It moves. It amplifies.
Pollution circulates according to urban morphology.
Climate change alters the dispersion of particles and intensifies heat waves.
Social inequalities determine who lives near congested highways and who benefits from tree-lined parks.
Transport infrastructures shape, every single day, the air our lungs absorb.
Everything is interconnected.
And yet, our scientific syntheses remain fragmented. They isolate determinants as if the city could be understood by slicing it into separate compartments.
It was this fragmentation that deeply challenged me.
How Urban Form and Mobility Patterns Shape Respiratory Health Risks 🏙️🚦
This research demonstrates that urban form and mobility patterns are key determinants of population exposure to air pollution and heat-related health risks, directly influencing respiratory health outcomes.
Based on a systematic review of 43 studies published between 2014 and 2024, the analysis identified 211 occurrences of risk factors associated with respiratory diseases in urban settings. The study applied a rigorous, multi-layered methodological framework combining PRISMA-based literature selection, structured data extraction, Natural Language Processing (NLP), multi-criteria weighting, statistical normalization, and validation through ANOVA and OLS models.
By integrating environmental, urban, and socioeconomic dimensions, the research provides a structured and reproducible approach to understanding urban health dynamics.
A key finding is that specific urban configurations can either exacerbate or mitigate respiratory risks. In other words, city design is not neutral: spatial organization and mobility systems directly shape exposure patterns and vulnerability.
The study ultimately highlights that urban planning is not only an infrastructural discipline but a fundamental component of public health strategy.
Breathing is a territorial act. 🌍🫁
This study does not claim to establish definitive causal relationships. Instead, it offers a framework for thinking differently.
To think of the city as an active determinant of health.
To see prioritization as a strategic tool.
To understand research as a bridge between disciplines.
Health is not built solely in hospitals.
It is built in neighborhood density.
In air quality.
In planning decisions.
In public policies.
Breathing is a biological act.
But breathing is also a territorial act.
And if we want healthier cities, we must accept a simple truth:
📐What we plan today will determine who breathes freely tomorrow. 🌍🌱
PhD in Territorial Dynamics, Urban Planning and Urban Governance at the National Institute of Urban Planning (INAU), Rabat. I hold a Master’s degree in Economic Analysis and International Development, with a specialization in Health Economics, from the University of Auvergne – CERDI (France).
Currently, I serve as a senior civil servant at the Regional Inspectorate of Urban Planning, Architecture and Territorial Development of Tangier-Tetouan-Al Hoceima. My work focuses on econometric analysis, medico-economic evaluation, territorial data analysis, urban development policies and urban health.
My research bridges public health, environmental and urban risk factors, and quantitative policy evaluation. I actively contribute to international collaborations and applied research initiatives.
Follow the Topic
-
Discover Public Health
This is an open access journal publishing research from all fields relevant to public health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Promoting Healthy Diets and Food Security across Global Public Health Systems
The interconnection between healthy diets and food security is a critical concern for global public health systems, particularly in the context of escalating population growth, climate change, and socioeconomic disparities. Proper nutrition is essential for overall health and well-being; however, millions worldwide face malnutrition in its various forms, including undernutrition, micronutrient deficiencies, and obesity. Food security encompasses not only the availability of food but also its accessibility, utilization, and stability. Addressing these complex challenges is vital for achieving sustainable development goals and improving health outcomes across diverse populations.
This Collection is motivated by the urgent need to strengthen the integration of health policy with healthy diet promotion and food security within public health frameworks. As nations work to build resilient health systems, innovative strategies that promote healthy eating and ensure food security are essential. This Collection aims to gather interdisciplinary insights and research that address these pressing issues, fostering collaboration among public health experts, nutritionists, policymakers, and community stakeholders.
The purpose of this Collection is to provide a platform for sharing research findings and practical solutions that enhance healthy diets and food security through effective health policies. We welcome contributions that explore policy interventions, community-based initiatives, and innovative programs focused on promoting nutrition education and improving food access. By highlighting diverse perspectives and successful models, this Collection seeks to inform future public health strategies and contribute to the development of effective, equitable food systems worldwide.
Topics of interest include, but are not limited to:
- Evidence-based community interventions to enhance food security
- The influence of health policy on food systems and public health outcomes
- Global case studies demonstrating effective food access and health promotion
This Collection supports and amplifies research related to SDG 2 and SDG 3.
Keywords: healthy diets; food security; nutrition promotion; malnutrition; public health; health policy; food access and availability
Publishing Model: Open Access
Deadline: Dec 05, 2026
The Economics of Longevity: Health Expenditure and Societal Implications for Public Health Systems
The relationship between health investment and life expectancy has long been a focal point in public health research and policy. As nations grapple with rising healthcare costs and varying health outcomes, understanding how financial allocations influence population health becomes increasingly critical. Numerous studies have illustrated that increased spending on health services often correlates with improvements in life expectancy; however, the complexities of this relationship are not fully understood. Factors such as socioeconomic status, healthcare accessibility, and the efficiency of health systems play significant roles in determining how investments translate into health outcomes.
At the national level, health investments primarily encompass government expenditure on healthcare systems, public health initiatives, and health infrastructure. Nations that allocate substantial resources toward healthcare often experience better health outcomes and increased life expectancy among their populations. For instance, countries with robust healthcare funding tend to provide more comprehensive services, including preventive care, chronic disease management, and health promotion programs, all of which contribute to enhanced population health. However, it is crucial to consider how these investments are distributed across different segments of the population. Inequities in health spending can exacerbate existing disparities, leading to significant differences in life expectancy among various demographic groups. Effective health investment strategies must address these disparities to ensure that improvements in life expectancy are equitable and inclusive.
The motivation for this Collection arises from the urgent need to bridge the gap between health expenditures and tangible improvements in life expectancy. Recent global health crises and ongoing disparities in health outcomes across different populations have underscored the necessity for a deeper exploration of how resource allocation affects health dynamics. This Collection seeks to provide a platform for researchers and practitioners to discuss empirical evidence, theoretical frameworks, and innovative approaches to understanding these critical interactions. By fostering dialogue around effective health investment strategies, we aim to contribute to the development of more equitable and efficient health systems worldwide.
The purpose of this Collection is to gather comprehensive research that elucidates the dynamics between health investment and life expectancy across diverse contexts. We welcome contributions that analyze historical trends, comparative studies, and policy evaluations, as well as those that explore the implications of financial investments on health equity. By highlighting interdisciplinary perspectives and fostering collaboration, this Collection aspires to advance the discourse on optimizing health investments for improved population health outcomes.
Topics of interest include, but are not limited to:
- Economic evaluations of health interventions
- Policy impacts on health spending and life expectancy
- Health equity and investment disparities
- Longitudinal studies on health expenditures and population health
This Collection supports and amplifies research related to SDG 3.
Keywords: health expenditure; healthcare economics; life expectancy; economic evaluation; population health; health investment; health policy
Publishing Model: Open Access
Deadline: Sep 04, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in