How long will you stay in the hospital if you have a complication after surgery? Results of a large study of across a broad range of surgical specialties and operations
Published in Surgery

Introduction
The amount of time someone spends in the hospital after surgery is important, both to the individual patient who wants to go home and to the healthcare system that needs to allocate beds and defray expenditures. But what aspects of your post-surgical course can affect the amount of time you might spend in the hospital after surgery? Right now, all studies in the literature focus on specific operations and have small samples sizes, potentially masking effects and resulting in imprecise estimates of effect size. This study aimed to answer that question using data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database across a wide spectrum of procedures and institutions.
What did we do?
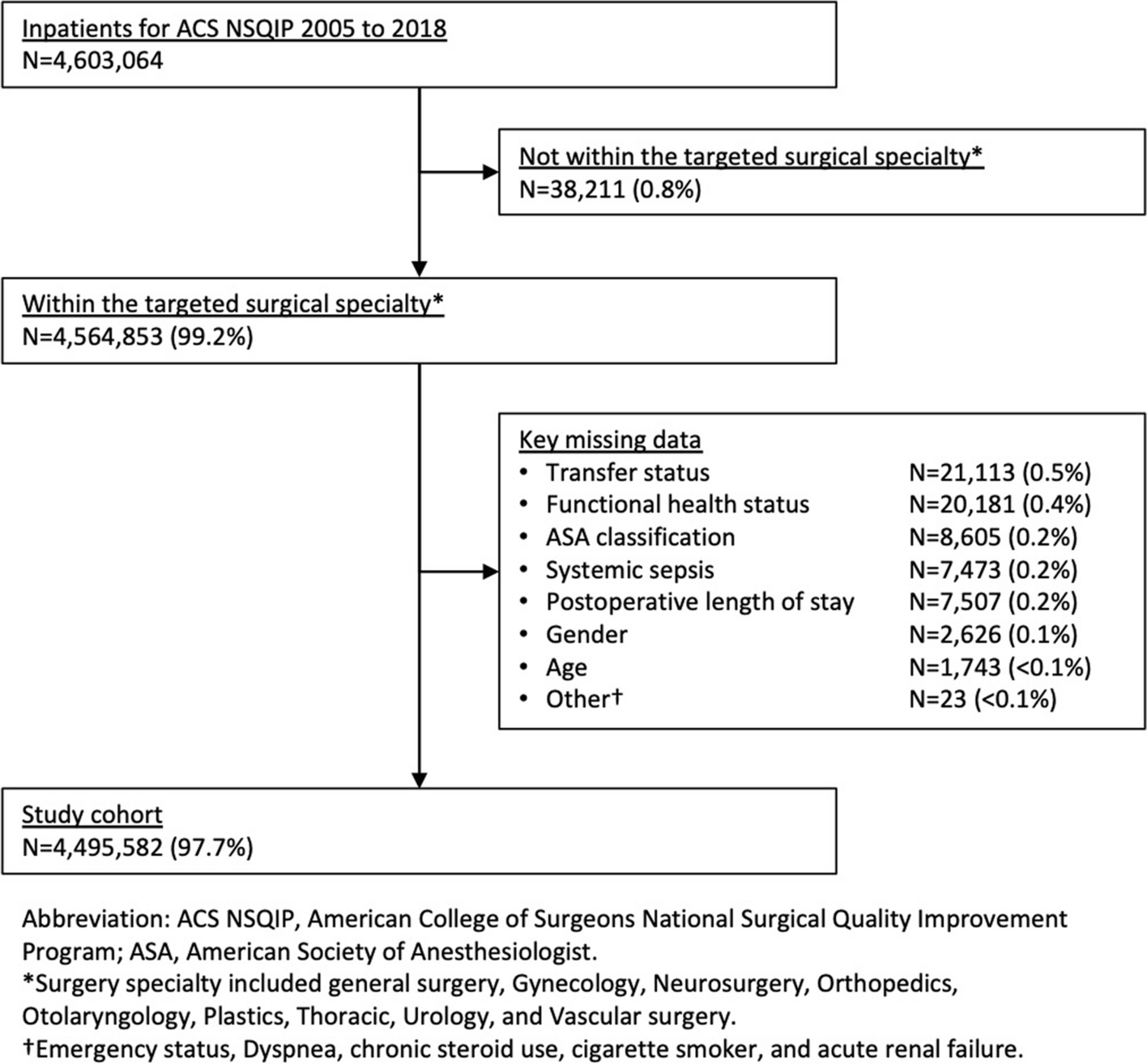
We analyzed data from patients undergoing inpatient operations in the large, national ACS-NSIP participant use file (PUF) database across nine surgical subspecialties (general surgery, gynecology, neurosurgery, orthopedic surgery, otolaryngology, plastic surgery, thoracic surgery, urology, and vascular surgery). We used preoperative characteristics and postoperative complications as the independent variables and postoperative length of stay as the dependent variable.
We examined the unadjusted association of each complication on postoperative length of stay. For this, we applied a Wilcoxon rank-sum test for variables with two categories, a Kruskal-Wallis test for variables with >2 categories, and a Pearson correlation coefficient for continuous variables. These statistical tests allow us to see the effect that each complication would have on a patient’s length of stay if they were to occur.
After we had those results, we wanted to adjust for the effect of other variables on each individual complication, because it is possible that having one complication, such as a urinary tract infection, makes another complication, such as sepsis, more likely. In addition, certain patient characteristics, such as having a chronic illness before surgery, may make the development of a complication after surgery more likely, but may have their own effect on length of stay. By controlling for these variables with a negative binomial model, we can isolate the attributable effect that each individual complication has on length of stay.
What did we find?
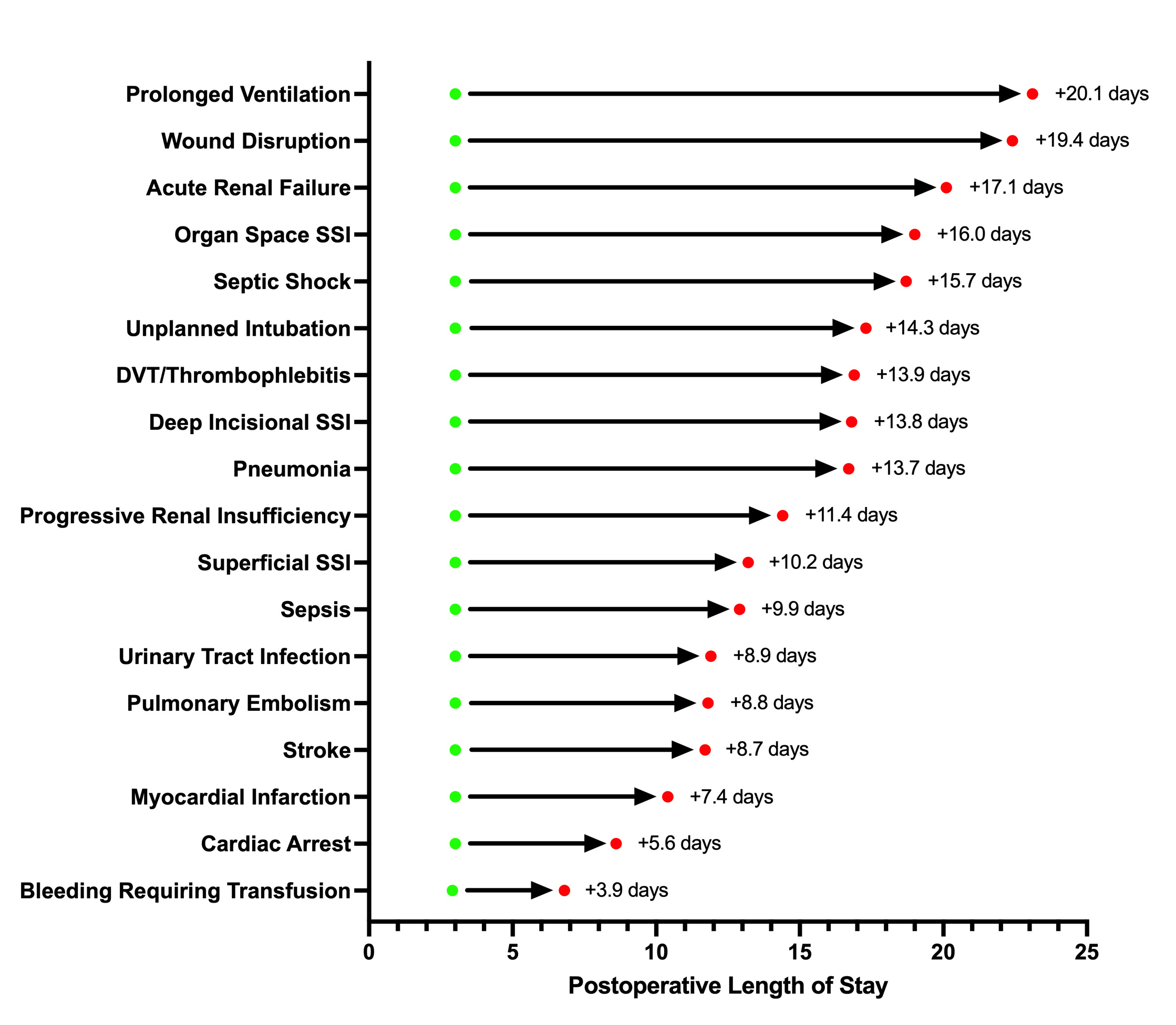
After controlling for all the considered variables, we found a statically significant correlation between time spent in the hospital postoperatively and development of any postoperative complication. The estimates of the magnitude of effect for each complication varied widely. The postoperative complication that had the largest individual effect on postoperative length of stay was prolonged postoperative mechanical ventilation, which increased length of stay by 20 days. Other complications with large effect sizes were wound disruption (increase of 19 days) and acute renal failure (increase of 17 days). In addition, we were able to find that certain patient characteristics had their own significant individual effect on length of stay; for example, underweight patients (BMI<18.5) ended up spending 2 days in the hospital more than patients in a BMI range of 18.5-24.9, and those who had ascites at the time of surgery spent 5 days longer in the hospital after surgery.
What can we do with this information?
This research and its conclusions have the potential to greatly improve patient counselling and healthcare/hospital resource management. If someone with dyspnea at rest is being worked up for and counseled about surgery and they want to know their recovery time, the surgeon can let them know that they will spend about 4 additional days on average in the hospital to recover. If a patient develops a pneumonia after surgery, they will spend an additional 14 days on average in the hospital. The findings of this study provide surgeons with a tool for additional preoperative counseling of patients. If a patient wants to know why quitting smoking before their surgery is important, a surgeon can let them know that smoking independently increases the time they would spend in the hospital, but it also increases their chances of developing respiratory complications, or poor wound healing, which could drastically increase the time they have to recover. Finally, these data can be applied on a large scale for quality improvement projects, targeting complications that have the greatest effect on length of stay, as well as improving bed allocations to prevent a shortage of beds in an acute care hospital from impacting the availability of services to critical patients. More research is needed to explore what quality improvement programs can help to reduce each high-impact postoperative complication, and thus what programs could most effectively reduce patient length of stay.
Take-home message
This study provides precise, actionable data that increases the toolkit of surgeons to counsel their patients on their hospital course, help patients have reasonable expectations about their postoperative length of stay in the event they develop a complication, and gives hospital administrators insight into where they should allocate their resources. Quality improvement programs that could prevent high-impact complications and improve bed allocation should be investigated, especially in an era of hospital staffing concerns.
Social Media
@garrett_healy @MeguidRobert
Follow the Topic
-
Patient Safety in Surgery
This is an open access journal that publishes articles on all issues related to safety and quality of patient care in surgery and surgical subspecialties.

Related Collections
With Collections, you can get published faster and increase your visibility.
New frontiers in patient safety for spine surgery
Spine procedures are inherently complex and carry significant risks, making safety a priority. As the field evolves, our commitment to improving patient outcomes, minimizing risks, and fostering a culture of safety remains critical. Recent advances in surgical techniques, robotics, navigation systems, artificial intelligence (AI), and minimally invasive approaches have revolutionized surgical practices and reduced recovery times, exemplifying the positive trajectory of this field of research.
As continued research is unlocking further innovations, this Collection seeks to engage scholars, clinicians, and healthcare professionals at the helm of innovation and improve outcomes and inform the wider audience. By addressing diverse topics related to safety practices, this Collection aims to foster a collaborative environment that enhances the overall quality of spine surgery and patient care.
Topics of interest for this Collection include but are not limited to:
- Innovations in surgical techniques
- AI in predictive analytics
- Minimally invasive spine surgery
- Patient safety culture in surgical teams
- Role of training and education in reducing errors
- Postoperative monitoring technologies
- Risk assessment and management strategies
- Patient engagement and decision-making
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Sep 02, 2026
Cutting edge innovation for patient safety in trauma surgery
We invite researchers to contribute to this special Collection. Topics of interest include but are not limited to:
- Innovative surgical techniques
- AI and machine learning in trauma care
- Telemedicine in surgical consultations
- Data analytics for outcome improvement
- Training simulations and educational technology
- Patient safety protocols and guidelines
- Robotics in trauma surgery
- Quality improvement initiatives
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Oct 16, 2026





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in