Laboratory capacity building during COVID-19 in Somalia: improving access to essential diagnostics for national health security in a fragile setting.
Published in Biomedical Research

The COVID-19 pandemic is remembered as a disease that has shaken the tenets of global health in a significant way. For over three years, from 2020 to 2022, it dominated as the leading cause of cases, hospitalizations, and deaths due to infectious disease, bagging the infamous title of the blockbuster virus of the decade. However, amidst the devastation, the pandemic exposed the underbelly of health security, exposing the gaps in preparedness, response, and recovery.
Additionally, due to limited countermeasures available in the early phase of the disease, testing and tracking infected individuals become the only available weapon to curtail transmission. This situation placed laboratories, a traditionally neglected sector of the healthcare system, at the center of the response. Indeed, it was time for the laboratory system to emerge from its neglect and assert its essential role in the health security landscape. While countries capitalized on this opportunity to develop their laboratory sectors, it was a particularly valuable opportunity for nations facing resource limitations and ongoing conflicts.
For the Federal Republic of Somalia, the scale-up of the infrastructure and health workforce capacities, along with the provision of state-of-the-art equipment and supplies achieved during this period, was unprecedented compared to any previous intervention from the government, humanitarian/development partners, or the private sector. These efforts were essential to expand access to testing for the population living in diverse settings, some of which were inaccessible due to insecurity. It was deemed important to share this experience through a scientific publication as a successful health program case study and to set a precedent for countries in similar contexts. Therefore, our articles illustrate how the opportunity was effectively utilized to transform the country’s laboratory system showing key milestones in the laboratory sector.
While similar narratives have emerged from other nations, such as Yemen, the context in Somalia differed fundamentally in several respects, some of which are described below:
Starting from scratch
Since the country is emerging from three decades of internal civil conflict, the central government continues to struggle to fulfill its statutory obligations, including providing essential healthcare. As a result, healthcare infrastructure is severely damaged due to years of neglect, the demand for services is overstretched, and the health workforce has limited capacity. Functional laboratories in the country were few and far between, making establishing capacities, especially at the State level, quite challenging owing to the lack of basic amenities like water and electricity.
The nightmare of non-state actors
The laboratory improvement program faced particularly significant challenges because it targeted a third of the population living in the precincts of de facto Non-State actors. Implementing health programs and testing services to hard-to-reach populations sometimes exposed us to risks. Ultimately, achieving the goal outweighed the fear, and the results justified the calculated risks.
Co-occurring health emergencies
The COVID-19 pandemic coincided with persistent outbreaks in the country, such as cholera and measles, which often diverted resources and focus, impeding implementation. Despite this, the global attention on COVID-19 at that time ensured that interventions to address the pandemic remained a top priority.
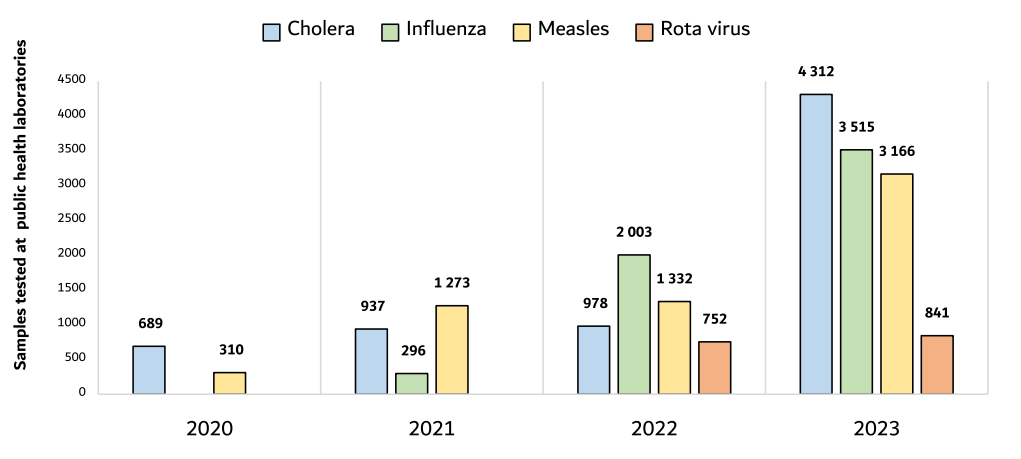
Of the many achievements reported in the paper related to laboratory and surveillance improvements, two main areas deserve a mention. First, laboratory capacity for molecular, bacteriological, and serological testing has been significantly expanded and improved to enhance surveillance of outbreak-prone diseases in the country. This development strategically positions the country’s public health laboratories on the road to recovery from many years of neglect. It also improves the country’s IHR core capacity and health security index score. Figure 1 below shows the progressive improvement in the number of tests for different endemic diseases.
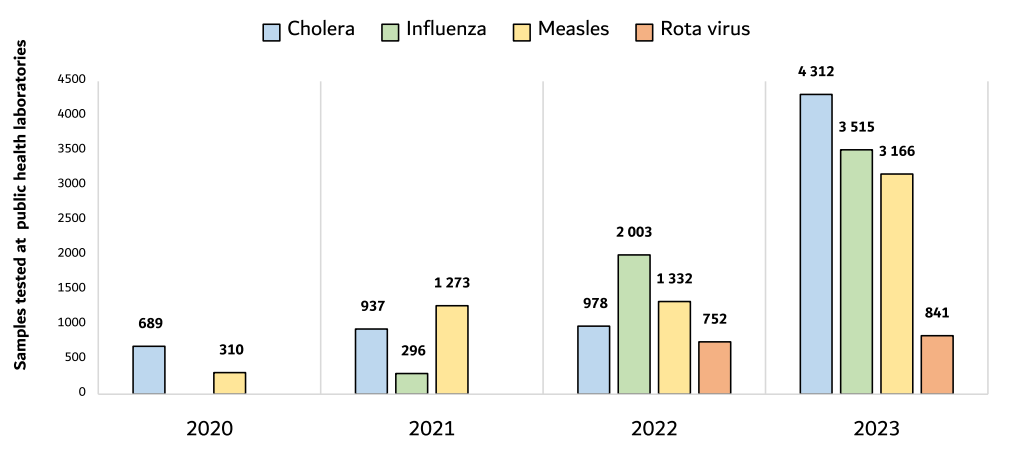
Figure 1: Showing the number of tests for different endemic diseases performed in public health laboratories between 2020 and 2023.
Second, establishing three genomic sequencing laboratories represents a transformative step toward access to innovative technologies, even in resource-limited settings. For countries reliant on humanitarian agencies for essential health programs, such as immunization programs, this kind of investment would typically be unfeasible during peacetime. However, the urgent necessity for in-country capacity to monitor circulating variants and the limited ability to refer samples outside the nation have underscored the importance of developing substantial local capabilities.
Next steps:
Establishing the infrastructure and installing the equipment are only a few pieces of the puzzle. The major task will be to sustain the progress and ensure the provision of the resources required to maximize the utilization of the established capacity. As interest in COVID-19 waned, complacency has already set in. However, to fill the gaps and ensure the functionality of this investment, leadership and prioritization in resource allocation will be required both at the MOH level and in critical health programs such as WHO.
In conclusion:
The COVID-19 pandemic was a lifetime opportunity for resource-limited, humanitarian-dependent countries to improve their laboratory systems. As reported in our article, this opportunity was well utilized in Somalia. The material infrastructure and human capacity built will be a national asset that will be useful for the generations to come. The lesson learned from COVID-19 should be a wake-up call for countries to prioritize investment in their laboratory systems for the safety and security of their population and as the first line of defense against infectious diseases. In the meantime, laboratory strengthening programs should be viewed as a critical and indispensable part of the healthcare system, even in the context of emergencies and resource limitations. Moreover, resources should be deliberately planned and allocated to ensure continuous improvement while sustaining the gains.
Parting shot—As leaders assemble for the World Health Assembly in Geneva between May 19th and 27th, 2025, to discuss global health issues, the role of laboratories in ensuring health security should be a standing agenda item followed by actionable resolutions. Indeed, the world should not wait for the next pandemic to realize the critical role laboratory programs play in ensuring health security for all.
Follow the Topic
-
Journal of Epidemiology and Global Health
The journal aims to impact global epidemiology and international health with articles focused on innovative scholarship and strategies to advance global health policy.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate and Environmental Change as Drivers of Infectious Disease: A Planetary Health Perspective
Human health is increasingly shaped by the interconnected pressures of climate change, environmental degradation, and socio‑ecological disruption. These planetary‑scale changes influence not only the epidemiology of infectious diseases, but also the public health systems, social structures, and community capacities that determine exposure, vulnerability, and resilience. This Collection adopts a planetary health perspective to explore how climate variability, ecosystem disruption, and human–environment interactions affect infectious disease risks and the public health responses needed to address them.
We welcome research that examines how shifts in temperature, precipitation, humidity, extreme weather events, land‑use change, biodiversity loss, and urbanization influence pathogen ecology, transmission pathways, and population vulnerability. Beyond epidemiological patterns, the Collection seeks contributions that address preparedness, surveillance, health system resilience, risk communication, governance, and cross‑sectoral interventions aimed at mitigating and adapting to climate‑related infectious disease threats.
Studies leveraging epidemiological datasets, climate and environmental records, spatial mapping, and predictive modeling are encouraged, as are qualitative, policy‑focused, and implementation‑oriented works that illuminate barriers and opportunities within public health systems. Particular attention is given to inequities in exposure and resilience, the needs of high‑risk populations, and the role of community‑level and institutional adaptation strategies.
By integrating epidemiology, environmental science, and public health practice, this Collection aims to advance understanding of climate–disease interactions, strengthen early warning and response systems, and inform adaptive strategies that protect and promote planetary health in a rapidly changing world. Topics of interest include but are not limited to:
- Climate‑sensitive infectious diseases and changing transmission patterns
- Impacts of extreme weather events and environmental disruption on disease risk
- Public health preparedness, surveillance, and early warning systems
- Health system resilience and climate adaptation strategies
- Socio‑ecological vulnerability, inequities, and community resilience
- Land‑use change, biodiversity loss, and zoonotic spillover
- Modeling climate, environmental, and disease interactions
- Governance, policy, and multisectoral responses to planetary health threats
- One Health and Planetary Health approaches to infectious disease prevention
This Collection supports and amplifies research related to SDG 13, Climate actions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 31, 2027
Public Health Professionals’ Education
Strengthening the education and continuous professional development of public health professionals is fundamental to achieving resilient, equitable, and responsive health systems. Recent global experiences including pandemics, protracted humanitarian crises, climate-related health risks, rapid urbanization, and technological transformation have highlighted both the critical role of the public health workforce and persistent gaps in training relevance, scale, quality, and sustainability. In many settings, educational models remain insufficiently aligned with real-world system needs, emerging competencies, and evolving career pathways.
While there is growing innovation in public health education, evidence and lessons learned are dispersed across disciplines and regions. A focused supplement in the Journal of Epidemiology and Global Health will provide a timely scholarly platform to consolidate high-quality research and practice-based insights.
The proposed Collection aims to advance knowledge in the education of public health professionals by:
Showcasing empirical evidence and innovative models for public health education and training
Examining how educational approaches align with health system priorities and workforce needs
Informing policy, institutional strategies, and investment in public health workforce development
Promoting equity, quality, and sustainability in public health education globally.
Scope and Thematic Areas
The supplement will invite original research articles, systematic or scoping reviews, and rigorously documented practice-based papers across the following thematic areas:
Competency-Based Public Health Education
- Core and advanced competency frameworks
- Alignment of curricula with population health needs and system priorities
Field-Based and Applied Learning Models
- Field Epidemiology Training Programs (FETPs) and similar applied training models
- Experiential learning, service-based education, and community engagement
Interprofessional and Multisectoral Education
- Collaborative training across health, social, environmental, and humanitarian sectors
- Preparing public health professionals for whole-of-government and whole-of-society approaches
Digital, Blended, and Distance Learning Innovations
- Online and hybrid training models
- Use of digital platforms, simulation, and emerging technologies in education
Education for Health Emergencies and Fragile Settings
- Workforce training for outbreak preparedness, humanitarian response, and conflict settings
- Adaptive education models in fragile and resource-constrained contexts
Equity, Ethics, and Inclusion in Public Health Training
- Gender, geographic, and socioeconomic equity in access to education
- Ethical dimensions of training, mentorship, and professional advancement
Leadership, Management, and Systems Thinking
- Training for public health leadership, governance, and policy engagement
- Building managerial and strategic competencies for system-level impact
Mentorship, Supervision, and Career Pathways
- Structured mentorship and supervision models
- Transition from training to practice and career progression
Monitoring, Evaluation, and Impact of Public Health Education
- Methods for assessing educational outcomes and workforce impact
- Long-term sustainability and return on investment of training programs
Partnerships, Financing, and Institutionalization
- Academic–government–partner collaborations
- Financing models and institutional integration of training programs
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 17, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in