Mechanism of acquired resistance to BRAF/MEK-targeted therapies in metastatic melanoma: Location, Location, Location?
Published in Cancer

Approximately ~50% of melanoma tumors are driven by activating mutations in BRAF, rendering these tumors susceptible to BRAF and MEK inhibition1. Among patients whose tumors harbor BRAF mutations, response rates to BRAF/MEK inhibition are observed to be as high as 68%. However, nearly 70% of patients will relapse within three years due to the development of acquired resistance2-4, and the underlying mechanism is unclear in many cases. BRAF inhibitors are reported to increase the infiltration of immune cells into the tumor microenvironment (TME) 5,6. The distribution of immune cells relative to each other as well as to tumor cells may influence not only melanoma disease progression, but also response to therapies7,8. Whether the interspatial distribution of immune and tumor cells predicts response to BRAF/MEK-targeted therapies and patient outcomes in melanoma is currently unknown.
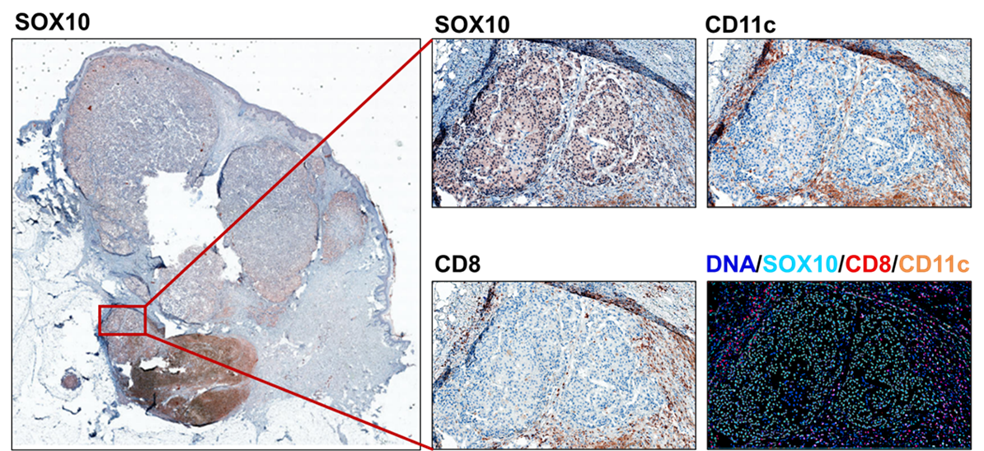
Our paper in NPJ Precision Oncology, using highly quantitative multiplex immunohistochemistry (MxIHC), the spatial distribution of immune and melanoma cells was quantified and correlated with clinicopathologic characteristics, response, and progression-free survival (PFS). Following progression of disease on BRAF/MEK-targeted therapy, surprisingly clinical resistance to therapy positively correlated with a close physical association between SOX10+ melanoma cells and CD8+ T cells. In the mouse BRAFV600E/PTEN-/- model9, we confirmed the detrimental role of the PD-L1:PD-1 axis in the interaction between melanoma-cells and CD8+ T cells. By further exploring the TCGA-melanoma dataset, tumor cellularity was confirmed to exhibit an additive prognostic value to the immune score signature in predicting overall survival (OS) in patients with early-stage melanoma. Moreover, tumor cellularity is prognostic for OS, independent of immune score in patients with late-stage melanoma. Our study highlights the fact that progression can occur despite a close proximity of CD8+ T cells to tumor cells and suggest that therapy resistant tumor cells are associated with production of an environment that inactivates the effector activity of tumor-proximal CD8+ T cells.
This study was a true collaborative approach developed by Chi Yan and Ann Richmond to understand mechanisms of drug resistance. We are fortunate to work with an excellent group of biostatisticians (Sheau-Chiann Chen and Gregory D. Ayers), clinical oncologists/physician scientists (Caroline A. Nebhan and Douglas B. Johnson), as well as experts in digital and clinical pathology (Joseph T. Roland and Vivian L. Weiss). Further studies are needed to decipher the crosstalk between rapidly proliferating melanoma cells and the effector activity of proximal CD8+ T cells. The poorer PFS in association with increased tumor cellularity could result from expansion of a treatment resistant clone which also has the capacity to inactivate the nearby immune effector cells. The mechanism by which the tumor cells influence the quantity and/or quality/phenotype of immune cells in the TME as well as their distribution and cellular interplay with immune cells remains an important question. These interactions likely contribute to acquired resistance of BRAF/MEK-targeted therapy.
References
1 Cancer Genome Atlas Network. Genomic classification of cutaneous melanoma. Cell 161, 1681-1696, doi:10.1016/j.cell.2015.05.044 (2015).
2 Long, G. V. et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet 386, 444-451, doi:10.1016/S0140-6736(15)60898-4 (2015).
3 Schadendorf, D. et al. Three-year pooled analysis of factors associated with clinical outcomes across dabrafenib and trametinib combination therapy phase 3 randomised trials. Eur J Cancer 82, 45-55, doi:10.1016/j.ejca.2017.05.033 (2017).
4 Robert, C. et al. Five-year outcomes with dabrafenib plus trametinib in metastatic melanoma. N Engl J Med 381, 626-636, doi:10.1056/NEJMoa1904059 (2019).
5 Borch, T. H. et al. Clinical efficacy of T-cell therapy after short-term BRAF-inhibitor priming in patients with checkpoint inhibitor-resistant metastatic melanoma. J Immunother Cancer 9, doi:10.1136/jitc-2021-002703 (2021).
6 Lelliott, E. J., McArthur, G. A., Oliaro, J. & Sheppard, K. E. Immunomodulatory effects of BRAF, MEK, and CDK4/6 inhibitors: implications for combining targeted therapy and immune checkpoint blockade for the treatment of melanoma. Front Immunol 12, 661737, doi:10.3389/fimmu.2021.661737 (2021).
7 Bosisio, F. M. et al. Functional heterogeneity of lymphocytic patterns in primary melanoma dissected through single-cell multiplexing. Elife 9, doi:10.7554/eLife.53008 (2020).
8 Gartrell, R. D. et al. Quantitative analysis of immune infiltrates in primary melanoma. Cancer Immunol Res 6, 481-493, doi:10.1158/2326-6066.CIR-17-0360 (2018).
9 Meeth, K., Wang, J. X., Micevic, G., Damsky, W. & Bosenberg, M. W. The YUMM lines: a series of congenic mouse melanoma cell lines with defined genetic alterations. Pigment Cell Melanoma Res 29, 590-597, doi:10.1111/pcmr.12498 (2016).
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Next-Generation AI in Drug Design for Precision Oncology
Publishing Model: Open Access
Deadline: Apr 01, 2027

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in