Most U.S. Babies Lack Key Gut Bacteria, Increasing Risk for Allergies and Other Chronic Health Issues
Published in Microbiology

Why This Research Matters: We’re getting sicker and sicker, at younger and younger ages.
As a mother and a scientist, my research aim is to improve the lives of all children, my own included. I co-founded Persephone Biosciences, with the mission of developing a technology platform to unlock the potential of the human gut microbiome for the prevention and treatment of disease. We started our microbiome research focused on cancer and how it influences treatment response in late-stage patients. Yet in 2021, one question broadened our focus: could our platform uncover the connection between infant microbiome and the alarming rise in noncommunicable diseases? This led to a connection with Dr. Richard Insel, a Pediatrician at the University of Rochester School of Medicine and Dentistry, whose involvement ignited the spark that set everything in motion — the decision to apply our innovative research approach to uncover infant dysbiosis and develop real solutions. The My Baby Biome study officially launched in August 2022.
The ‘first 1,000 days’ is a well-documented time frame in which lifelong health, or disease, is established. It has become increasingly clear that the early microbiome plays a critical role, and disruption in the gut microbial community is likely a driving force behind the rise in chronic illness. The CDC reports that 6/10 young adults have a chronic disease, and in the last 10 years, prevalence in this population has risen by 7%. Similar findings are reported in pediatrics, with approximately 40% of children and adolescents having a chronic condition. Especially notable is the rise of eczema and its progression to food allergies and asthma, known as the atopic march.
Despite increasing rates of health conditions and evidence pointing to the microbiome as a key mediator, research on the state of the infant gut is lacking. The goal of the My Baby Biome study is to provide comprehensive characterization of the infant microbiome, insight into the prevalence of dysbiosis in early life, and identify key mediators for atopic march health outcomes.
Ultimately, this data can help develop novel restorative interventions to address widespread infant microbiome dysbiosis and reduce immune-related health conditions in the pediatric population and beyond.
The My Baby Biome Approach: The largest and most accurate study to date
A hallmark of the My Baby Biome study is its size and population representation. This study is the largest of its kind in the U.S., including 412 infants, an over 80% increase in size over the largest similar study. Representing 48 of 50 states and racial composition reflective of the U.S. population, this cohort is a true reflection of U.S. infants, a feature lacking in previous research. Further, the study will follow participants until 7 years old, allowing for association between early microbiome and health outcomes.
Another unique aspect of My Baby Biome is the inclusion of babies born by vaginal and C-section deliveries, and feeding mode tracking - breastmilk, formula or mixed. These are common microbiome influencers and their inclusion is key for translating the findings from this study to all infants.
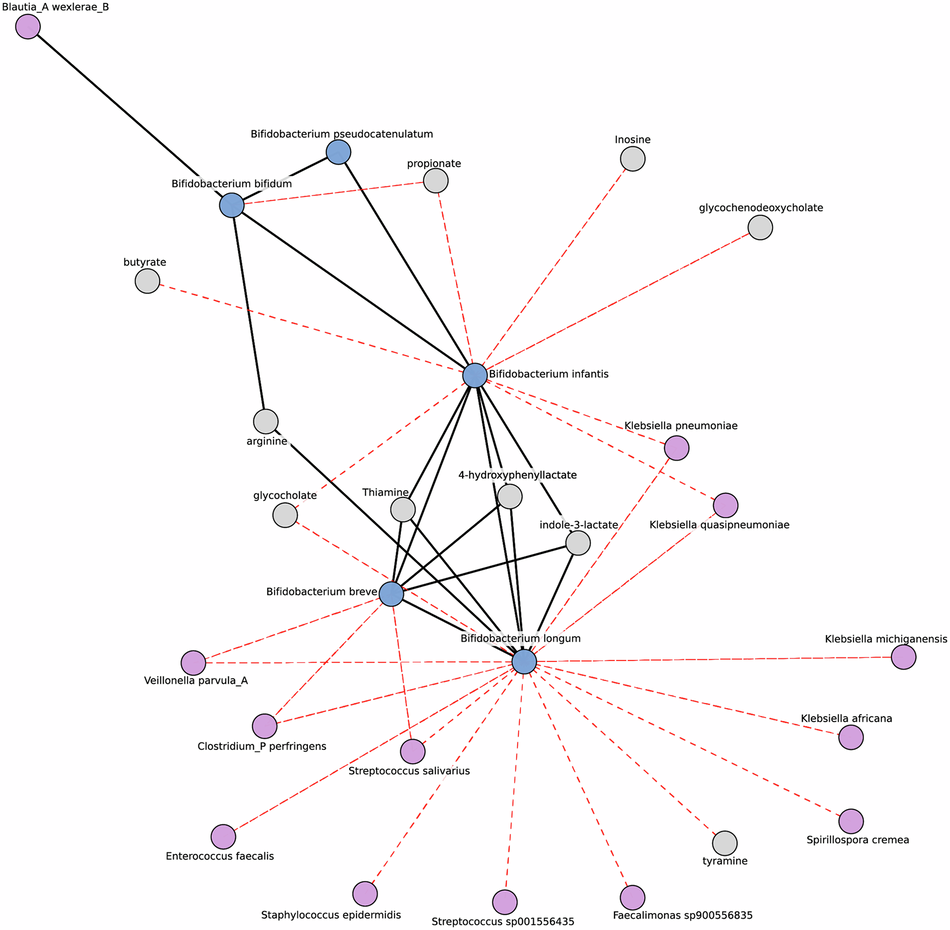
The use of shotgun metagenomics rather than dated technologies like 16S also sets the My Baby Biome study apart by allowing us to assess not only which microbes were present or absent in the microbiome with extreme accuracy, but also microbial functional capacity. We also measured key metabolites and using our in-house A.I.-driven technology platform, we generated a microbe-metabolite network analysis. This has resulted in the largest, most comprehensive, in-depth, and accurate characterization of the U.S. infant gut.
Key Findings: 9 out of 10 infants are missing a critical microbe
The key result from My Baby Biome is the discovery that 92% of infants are missing Bifidobacterium infantis - the most important microbe species for infants. Furthermore, 25% are missing Bifidobacterium species overall. Missing Bifidobacterium is an issue present in infants from all delivery modes and feeding methods, not only for C-section and formula-fed babies as previously assumed.
The microbiomes of the infants studied fell into one of three community states:
|
Community state |
Microbiome Composition |
Percentage of Infants |
Clinical associations |
|
C1 |
Bifidobacterium dominated |
24% |
Breastfeeding |
|
C2 |
Bifidobacterium longum present Dominated by Bacteroidota |
37% |
Vaginal delivery |
|
C3 |
High abundance of Firmicutes and Proteobacteria
C. perfringens is the most abundant microbe
Minimal to absent Bifidobacterium |
39% |
C-section delivery |
C1 is the ideal community state and is associated with high abundance of HMO consuming Bifidobacterium, whereas C2 and C3 have reduced HMO-digestion capacity, higher gut pH, and higher virulence factor and antimicrobial resistance genes.
A shocking 76% of infants in the study fell into C2 or C3 categories. At two years old, infants with these microbiomes were three times more likely to have atopic march conditions compared to C1. The abundance of Bifidobacterium had the opposite impact, with a 3.1 times risk reduction for negative health outcomes as a function of Bifidobacterium abundance.
These data provide strong evidence for early microbiome dysbiosis as a driving factor in atopic march condition development, and Bifidobacterium as a mediating microbe in this interaction. In other words, we’re learning what our babies need to get back on track.
Broader Implications: Infant dysbiosis may be the root cause of atopic march (and even cancer).
The findings of the My Baby Biome so far are alarming, demonstrating increased risk of adverse immunological outcomes following dysbiosis, as early as two-years old. Other research continues to uncover the link between early microbiome disruption and later health outcomes. Of particular interest to Persephone given its roots in studying the microbiome’s role in cancer therapeutics, a recent groundbreaking study by Diaz-Gay, et al found that early life microbial production of colibactin toxin by certain E. coli strains may pave the way for early-onset colorectal cancer. With the rising rate of chronic illnesses starting at increasingly younger ages, including cancers, the microbiome is a critical target for intervention.
Stephanie Culler, PhD, co-founded Persephone Biosciences in the summer of 2017 with the mission of developing a technology platform to unlock the potential of the human gut microbiome for the prevention and treatment of disease. Through Persephone’s Poop For The Cure® clinical research program, she initially focused on investigating the gut microbiome’s role in treatment response among advanced-stage cancer patients, with the goal of developing a microbiome-based cancer therapeutic.
In December 2021, the potential of the platform expanded when emerging insights revealed an opportunity to address infant gut dysbiosis — a condition increasingly linked to adverse long-term health outcomes. Persephone became dedicated to solving this global health crisis, leading to the launch of the My Baby Biome study in August 2022.
Follow the Topic
-
Communications Biology
An open access journal from Nature Portfolio publishing high-quality research, reviews and commentary in all areas of the biological sciences, representing significant advances and bringing new biological insight to a specialized area of research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Dec 31, 2026
DNA repair and human disease
Publishing Model: Hybrid
Deadline: Oct 31, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in