Overcoming the Challenges in Managing the Deadly Hepatitis Delta Infection
Published in Healthcare & Nursing and General & Internal Medicine
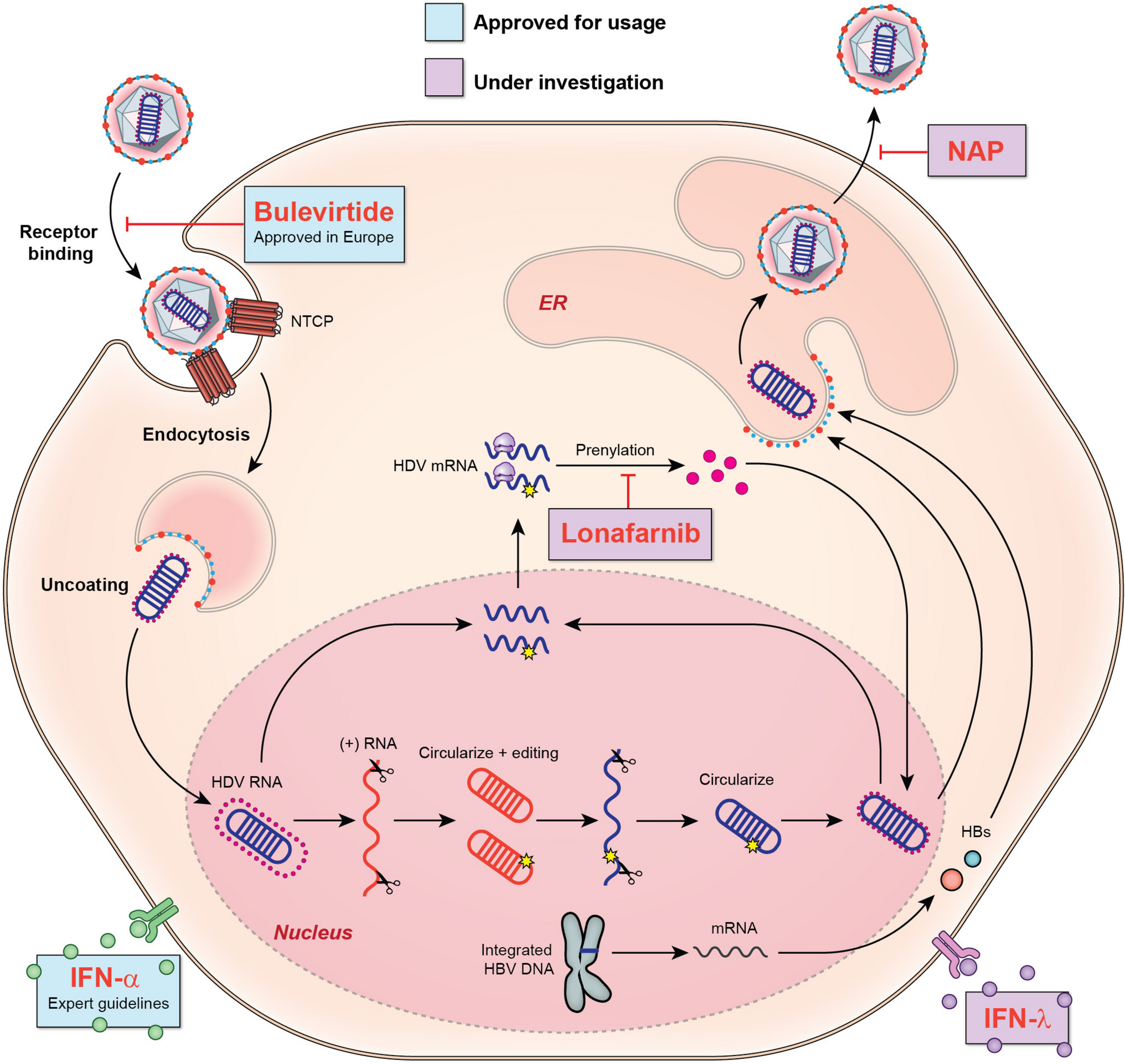

First discovered in 1977, the Hepatitis D virus (HDV) is the smallest known pathogenic virus affecting humans. This defective RNA virus uniquely relies on the Hepatitis B virus (HBV), particularly the hepatitis B surface antigen (HBsAg), for its transmission and the human host for its replication. Despite its small size, HDV is highly potent, often causing rapid liver disease progression to cirrhosis and significantly increasing the risk of hepatocellular carcinoma (HCC). HDV is also genetically diverse, encompassing eight genotypes with 2 to 4 subtypes each, with genotype 1 being the most prevalent globally. Current estimates suggest that HDV affects approximately 12-15 million people globally, making it a major public health concern. However, the actual prevalence of HDV may be much higher due to underutilized screening tests. Limited awareness and understanding of this aggressive infection underscore the urgent need for improved education and comprehensive screening efforts to tackle this serious global health threat.
HDV is primarily transmitted through the parenteral route, with intravenous drug users at the highest risk for its transmission. HDV is significantly more prevalence in certain regions like Mongolia, Western and Central Africa, and Eastern Europe, referred to as "hotspots." HDV can infect individuals in two distinct ways: as a "superinfection" in those already infected with Hepatitis B, or as a "co-infection" occurring simultaneously with HBV transmission. While co-infections are typically acute and self-limiting, a staggering 90% of superinfections progress to chronic HDV. Identifying whether an infection is acute, chronic, a co-infection, or a superinfection can be challenging. Our review (Table 1) discusses serological testing to accurately identify the disease state.
The American Association for the Study of Liver Diseases (AASLD) currently recommends screening only high-risk groups with HBV for HDV. In contrast, European and Asian associations advocate for testing all HBV patients for HDV. Recent studies indicate that universal screening of all HBV patients is essential to accurately gauge the prevalence of HDV. This has led to a push for reflex anti-HDV antibody testing in HBV patients to improve screening. However, the lack of standardized testing remains a significant limitation for diagnosing HDV, as confirmatory PCR testing is not standardized, and current PCR assays show variability in accuracy across different HDV genotypes. Additionally, there is no systematic method for screening, assessing disease severity, and conducting surveillance, further complicating the management of HDV. To assist clinicians in providing care to HDV patients, we have created a schematic diagram (Figure 2) in our review. While liver biopsy is generally considered necessary to assess disease severity in chronic hepatitis D patients, noninvasive imaging methods, such as vibration-controlled transient elastography, have proven to be reliable in distinguishing patients with and without advanced liver disease.
Because HDV relies on the host for most of its replicative life cycle, targeting antiviral therapies is highly challenging, adding to the complexity of treatment. Consequently, there are currently no medications that are both effective and safe in eliminating HDV. Hence current guidelines recommend - for finite therapy (less than 48 weeks), the primary endpoint is the loss of HBsAg maintained for at least 24 weeks after stopping treatment. For maintenance therapy (more than 48 weeks), the goal is to achieve HDV RNA levels below the lower limit of quantification (LLOQ). Although existing medications, both old and new, can decrease the viral load, most patients experience relapse once the medication is discontinued. Therefore, alternative endpoints for finite treatment include HDV RNA levels below LLOQ 24 weeks off treatment. For maintenance therapy, the goals are a ≥2 log IU/mL decline in HDV RNA compared to baseline and normal ALT levels. These complexities in treatment goals underscore the challenges we currently face in our efforts to eliminate this deadly infection. Recent article which involved combination of two drugs bulevirtide (an entry inhibitor) and peg interferon (immunomodulator) showed that the combination is better that individual drugs.
Currently, there is no vaccine for HDV, leaving individuals with HBV particularly vulnerable. Although universal vaccination for HBV has decreased the number of HBV and HDV infections, the uptake rate has been suboptimal, resulting in continued vulnerability to both. Increasing HBV vaccination rates is one of the most effective strategies to prevent disease transmission. In addition to vaccination, we should focus on identifying the true prevalence of HDV by raising awareness about the virus. It is also crucial to understand the factors that leads to the rapid progression of HDV to cirrhosis and HCC and to determine ways that can help identify individuals at risk for disease progression. The ultimate goal of HDV management remains eradication of HDV, and while significant strides have been made in managing the virus, continued efforts are essential to achieving this goal.
As we observe World Hepatitis Day, let us take a moment to celebrate the progress we've made and strategize our next steps towards a world free of hepatitis.
Follow the Topic
-
Current Hepatology Reports
This journal intends to provide clear, insightful, balanced contributions by experts, that review the most important recently published clinical findings related to the study, diagnosis, treatment, management, and prevention of acute and chronic liver disease.

Related Collections
With Collections, you can get published faster and increase your visibility.
Topical Collection on Fatty Liver Disease
Publishing Model: Hybrid
Deadline: Ongoing
Topical Collection on Management of the Cirrhotic Patient
Publishing Model: Hybrid
Deadline: Ongoing


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in