Rate and predictors of loss to follow-up in HIV care in a low-resource setting: analyzing critical risk periods
Published in Biomedical Research


Why Do Some People Stop HIV Treatment? Understanding the Key Moments
In the global fight against HIV, keeping people engaged in their treatment is crucial. Even though many countries aim to meet ambitious HIV care goals by 2030, a significant challenge remains: helping those who start HIV treatment continue their care and keep their virus under control. A big part of this challenge is what’s known as "loss to follow-up" (LTFU).
What is Loss to Follow-Up (LTFU)?
LTFU happens when someone on HIV treatment misses their medical appointments or stops taking their medication for over 28 days. This is a serious issue, as it can lead to poorer health, increased risk of death, and a higher chance of spreading HIV to others because the virus isn’t being suppressed.
When Do People Stop Treatment?
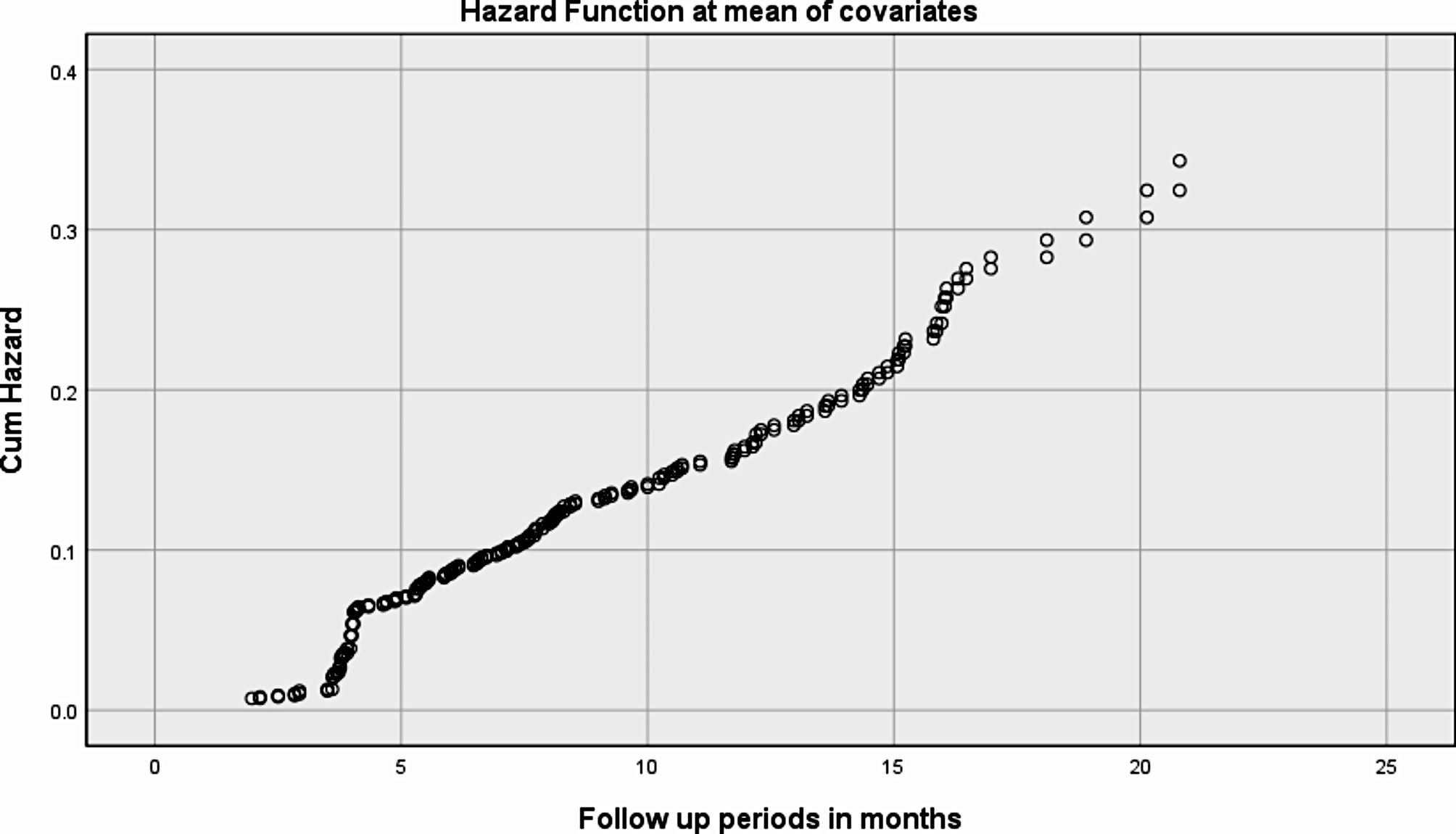
This study looked at 737 adults who were new to HIV care and identified the times when they were most likely to stop their treatment:
- The First 6 Months Are Critical: About 50% of the people who dropped out of care did so within the first six months. This early period is a high-risk time, with an LTFU rate nine times higher than later periods (13-24 months). People might face challenges like dealing with side effects, struggling to adjust to a new routine, or not yet seeing the benefits of the medication.
- 7-12 Months: A Continued Risk: Even though the risk of dropping out decreases after the first six months, many people still struggle to stick with their treatment during months 7-12. About 30% of those who stopped care did so during this time. Factors like financial difficulties, stigma, or transportation issues can continue to affect them.
- After 12 Months: A More Stable Phase: After a year on treatment, the dropout rate drops significantly. By this time, many patients have adjusted to their routine, seen improvements in their health, and are more committed to their treatment.
What Can We Do About It?
The findings suggest that the first six months of HIV treatment are a make-or-break time. Health programs should focus on providing extra support during this period, such as helping patients manage side effects and offering counseling. Continued support is also important in the following months to help people overcome challenges that might come up later.
Follow the Topic
-
BMC Infectious Diseases
This journal is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of infectious and sexually transmitted diseases in humans, as well as related molecular genetics, pathophysiology, and epidemiology.

Related Collections
With Collections, you can get published faster and increase your visibility.
Tropical vector-borne infectious diseases
BMC Infectious Diseases is calling for submissions to our Collection on Tropical vector-borne infectious diseases.
Tropical vector-borne infectious diseases represent a major global health challenge, particularly in low- and middle-income countries. Transmitted by vectors such as mosquitoes, ticks, and flies, these diseases include well-known conditions like malaria, dengue fever, and leishmaniasis, as well as neglected tropical diseases. Their transmission dynamics are shaped by a complex interplay of environmental, climatic, social, and behavioral factors, making integrated and interdisciplinary research essential for effective control and prevention.
Addressing these diseases is vital not only for the health of affected populations but also for global health security. Recent advances in surveillance, vector control, therapeutics, and vaccines have improved our ability to respond to outbreaks. However, continued research is needed to understand the mechanisms of disease transmission, predict emerging threats, and implement effective interventions in diverse tropical settings.
This Collection welcomes original research articles on, but not limited to, the following topics:
- Mechanisms of disease transmission in tropical environments
- Mechanisms of vector-borne disease transmission and vector-parasite-host interactions.
- Emerging tropical pathogens and their impact on human and animal health
- Surveillance strategies, including genomic, climate-informed, and digital approaches
- Vector control strategies and evaluation of their effectiveness
- Epidemiological and mathematical modeling of vector-borne diseases
- One Health approaches linking humans, animals, and the environment
We encourage interdisciplinary submissions that advance understanding of vector-borne disease dynamics and support the development of innovative, data-driven strategies for disease prevention, control, and global health resilience.
This Collection supports and amplifies research related to SDG 3 (Good Health and Well-being).
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Nov 13, 2026
Tuberculosis and co-infections: diagnostics, management, and treatment
BMC Infectious Diseases invites submissions for a Collection on Tuberculosis and co-infections: diagnostics, management, and treatment.
Tuberculosis (TB) remains a leading cause of morbidity and mortality worldwide, particularly in regions with high prevalence rates and co-infections. The interplay between TB and various co-infections (including bacterial, viral, parasitic and fungal), complicates diagnosis and treatment strategies. Advances in molecular diagnostics and imaging techniques have improved our understanding of how these co-morbidities affect TB pathogenesis and treatment outcomes. However, the challenge of managing drug-resistant TB adds an additional layer of complexity, necessitating a comprehensive approach that integrates the latest research findings with clinical practice.
Research into TB of all stages and its co-infections is crucial for addressing the rising incidence of drug resistance and improving patient outcomes. Recent studies have identified critical biomarkers for early detection and prognosis, highlighting the role of rapid diagnostic tools in the clinical setting. Additionally, understanding the mechanisms of co-infections has led to tailored treatment regimens that maximize efficacy while minimizing adverse effects. Nonetheless, gaps remain in our knowledge of optimal management strategies for these complex cases, emphasizing the need for ongoing research in this field.
Future research endeavors should focus on the development of more effective diagnostic techniques and treatment protocols that consider the multifaceted interactions between TB and its co-infections. Innovations in personalized medicine may lead to targeted therapies that address specific pathogen interactions, ultimately enhancing patient recovery rates. Moreover, collaborative efforts between public health entities and research organizations could pave the way for comprehensive TB surveillance systems, fostering the identification of emerging trends in co-infection patterns.
This Collection welcomes original research articles on topics including but not limited to:
- Diagnostic innovations for Tuberculosis and co-infections
- Management strategies for drug-resistant Tuberculosis
- Interaction between Tuberculosis and HIV
- Tuberculosis and diabetes comorbidity
- Tuberculosis in the context of viral hepatitis and COVID-19
This Collection supports and amplifies research related to SDG 3 (Good Health and Well-being).
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 27, 2027
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in