
Have you ever touched nettles and developed nasty, itchy red spots on the skin?
This is what is called urticaria, derived from the latine root Urtica, ortie in French, nothing more than the translation of nettles. Could you imagine living with a chronic condition that would cause such prickling rashes to appear anywhere on your body without warning for more than six weeks? This medical illness exists and is called chronic urticaria. It affects 0,2-1% of the population, and has major outcomes on life quality, similar to that reported for patients awaiting coronary-artery bypass grafting (1)(2). This condition can unfortunately last for several years (2). CU can be classified as spontaneous or inducible. In the last condition, CU is triggered by physical factors such as temperature, touch, vibration, sun, cholinergic activity, pressure or contact. (2)
But what is exactly the mechanism hiding behind it and its causes? And how has the SARS-Cov2 pandemic led our group to contribute to its understanding?
Chronic urticaria (CU) and its Etiology
CU pathogenesis has still not fully been elucidated. Yet, two major hypotheses are commonly acknowledged, which both result in the chronic degranulation of mast cells, the primary cell type involved in allergic reactions (3). In one condition, the body develops specialized antibodies (IgE), normally associated with an allergic reaction but redirected against self-antigens, such as hormones (4). In the second condition, the body develops an antibody-mediated (IgG) autoimmune disease redirected against the surface receptors of mast cells.
Importantly, urticaria flares are likely the result of the cumulation of predisposing factors revealed by diverse facilitating factors, such as non-steroid anti-inflammatory drugs, acute (including SARS-Cov-2) and chronic infections (e.g helminths, H.pylori, hepatitis), stress, but also autoimmune diseases.
From the first observations to the initiation of the Study
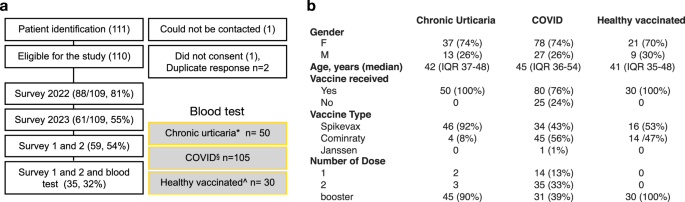
Our work was initiated as an independent observation made in early 2022 by us and some local allergists of CU cases, which were temporally related with the administration of the mRNA COVID-19 vaccine booster. To rapidly confirm this observation, we established an online survey that was open to any patient who was diagnosed with CU after vaccination by any of the local allergists from the GVAIC association (Groupement Vaudois des allergologues et immunologues), and could rapidly recruit 88 patients. We first confronted these results at a national level to those reported to the Pharmacovigilance Unit of Swissmedic. We found very similar results with an overall crude incidence rate of CU after a COVID-19 booster at 19/100’000 from 2021-01-21 to 2022-08-31 (5). In our cohort, about 90% of the new-onset of CU started after the Moderna mRNA-1273 vaccine (Spikevax) vaccine in middle-aged (40-year-old) of female predominance. Strikingly, the median time between the booster and the onset of CU was 10 days, roughly corresponding to the time for initiating an immune response.
As the onset of CU corresponded to the same period of many COVID-19 infections, COVID-19 disease could have represented an important confounding factor. Additionally, considering the low prevalence of CU after the booster, it remained unclear whether there was a directed causality between the vaccine and the onset of CU, particularly whether an allergy to the vaccine could explain the onset of CU (6). Therefore, about a year later, we conducted a follow-up survey and proposed to 50 patients a blood test for better characterization of the disease over time.
Main results of our study
To address the contribution of COVID-19 to the onset of CU after vaccination, we first aligned epidemiological data comparing vaccination date, onset of CU, and COVID-19 disease in the general population. We observed that the pick of CU cases preceded the pick of COVID-19 reports and was shifted compared to the vaccination peak. These data were also confirmed in patients with CU, as no temporal correlation could be made between the CU onset and COVID-19 disease. Importantly, patients exposed to SARS-COV-2 (confirmed by blood testing) had neither a more severe disease, nor a more prolonged disease.
To understand whether CU patients had developed allergic antibodies (=sensitization) directed against one of the vaccine excipients (mainly Polyethylene glycol), commonly found in many cosmetics, drugs and even foods, we performed a functional blood test. To validate such results, we had to include a large number of control patients (n=135) without CU. Our results showed that CU patients were not more sensitized against the vaccine excipients than the control population nor that a sensitization was associated with a more prolonged disease. Interestingly, however, we found that patients who received the Spikevax booster clearly had a higher vaccinal response and a higher chance of being sensitized against its excipients. The relevance and persistence of such sensitization remain unclear. Therefore, as of today, no recommendations/precautions are made by the expert societies.
Tolerance to vaccine reexposure and hypothesis for pathogenesis of CU after booster
Four patients with CU after the vaccine received a novel vaccine injection (3 with Comirnaty, 1 Spikevax), yet no flare or recurrence of urticaria was observed. Although this is a limited number of patients, these results suggest that mimicry mechanisms by which antibodies would cross-react between self-antigen and the vaccines are not involved. This would indeed explain the low frequency of CU after the booster. However, considering that 10 days are needed between the booster and the start of CU, these results suggest that the vaccine provides a favorable condition and environment to develop CU in predisposed patients. Thus, the vaccine should not be considered an inducer but a facilitator of a disease highly prevalent in the general population.
Take Home Message
Our study should not discourage people from receiving a vaccine, particularly the elderly and immunosuppressed patients, for whom no cases of CU have been reported to the best of our knowledge. For those who start CU, since a formal etiology, cannot be identified in most cases and because specific biomarkers are still poorly developed, it is essential to rapidly start non-sedative antihistamines, which can be prescribed up to four times a day to control the burden of symptoms. Thus, the management of post-vaccination CU should follow previously established guidelines as for other forms of CU.
Bibliography
- Maurer M, Abuzakouk M, Bérard F, Canonica W, Oude Elberink H, Giménez-Arnau A, et al. The burden of chronic spontaneous urticaria is substantial: Real-world evidence from ASSURE-CSU. Allergy. 2017 Dec;72(12):2005–16.
- Lang DM. Chronic Urticaria. N Engl J Med. 2022 Aug 31;387(9):824–31.
- Kolkhir P, Muñoz M, Asero R, Ferrer M, Kocatürk E, Metz M, et al. Autoimmune chronic spontaneous urticaria. J Allergy Clin Immunol. 2022 Jun;149(6):1819–31.
- Sánchez J, Sánchez A, Cardona R. Causal Relationship Between Anti-TPO IgE and Chronic Urticaria by In Vitro and In Vivo Tests. Allergy Asthma Immunol Res. 2018 Oct 12;11(1):29.
- Duperrex O, Tommasini F, Muller YD. Incidence of Chronic Spontaneous Urticaria Following Receipt of the COVID-19 Vaccine Booster in Switzerland. JAMA Netw Open. 2023 Feb 1;6(2):e2254298.
- Pescosolido E, Muller YD, Sabaté‐Brescó M, Ferrer M, Yerly D, Caubet J, et al. Clinical and immunological data from chronic urticaria onset after mRNA SARS‐CoV‐2 vaccines. Clin Exp Allergy. 2022 Aug 23;10.1111/cea.14214.
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Exercise and Physical Activity in Health and Disease
Publishing Model: Open Access
Deadline: Sep 03, 2026
Life Course Epidemiology
Publishing Model: Open Access
Deadline: Sep 30, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in