Sex differences research is important!
Published in Sustainability and General & Internal Medicine

Co-published today, May 13, in recognition of Sex Differences in Health Awareness Day, this Q&A accompanies the Editorial: Sex still matters for the brain and mental health across the lifespan and the Review Article: The role of sex differences in cardiovascular, metabolic, and immune functions in health and disease: a review for “Sex Differences in Health Awareness Day”—both co-authored by members of our Editorial Board. This Q&A also highlights a recent Editorial by our Editor-in-Chief, Dr. Jill Becker, and Dr. Sofia Ahmed, titled Sex differences research is important!, written in response to recent federal funding cuts and the elimination of key information resources—developments that underscore the urgent need to prioritise and protect sex differences research.

Could you begin by telling us about yourself and your role at the Organization for the Study of Sex Differences? How does your work align with the goals of Sex Differences in Health Awareness Day?
I am a nephrologist and clinician-scientist in the Faculty of Medicine & Dentistry at the University of Alberta in Edmonton, Canada. I also serve as the Academic Lead for Women’s Health Research at the Women and Children’s Health Research Institute and as President of the Organization for the Study of Sex Differences.
Some of the goals of Sex Differences in Health Awareness Day include raising awareness of health disparities and differences in how certain conditions—such as heart disease, autoimmune disorders, and substance use disorders—manifest differently in men and women. Recognizing sex differences is crucial for accurate diagnosis and effective treatment and the first step to accomplishing this is rigorous, reproducible, and inclusive research. Encouraging the adoption of healthcare approaches that consider sex and gender differences ensures that everyone receives appropriate care tailored to their specific needs.
What is the primary focus of your research, and can you share examples of how the same disease may present differently in men and women?
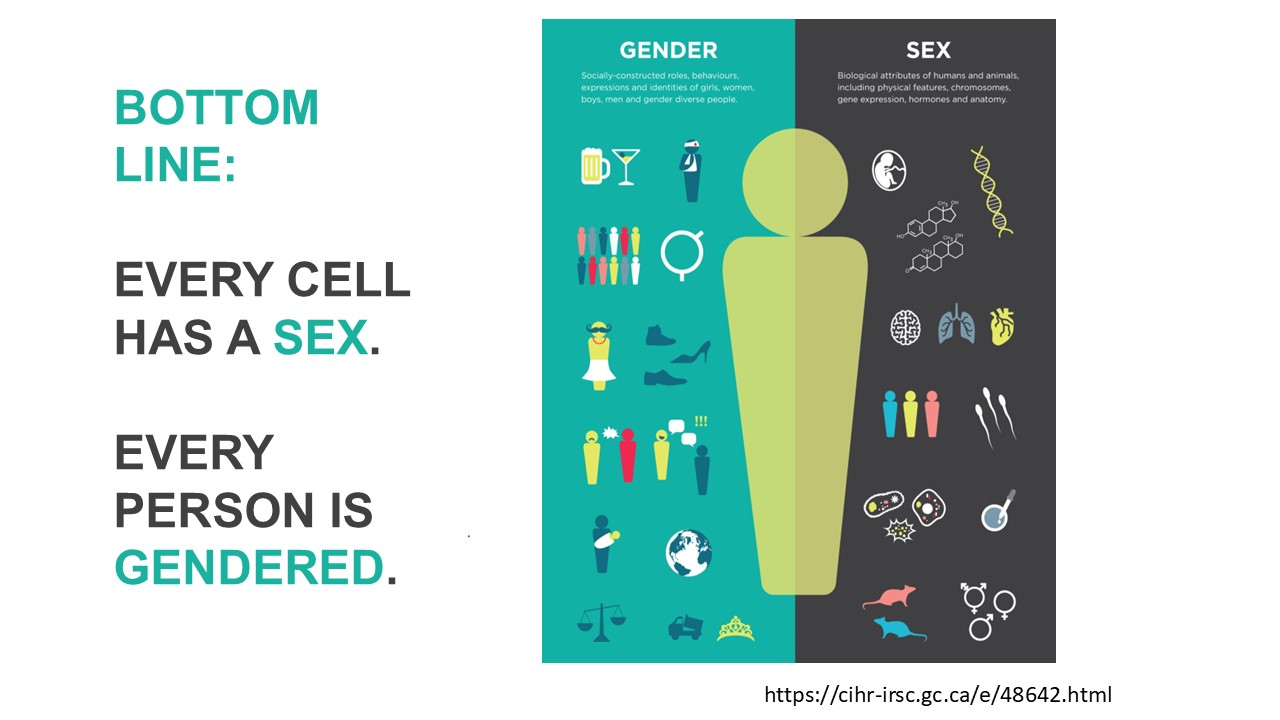
My program of research is focused on how sex (biological attributes) and gender (sociocultural factors) affect kidney and cardiovascular physiology and health outcomes. Women develop cardiovascular complications at a lower blood pressure than do men, however at present there is a single target blood pressure used in clinical management. Moreover, specific sex-specific events across the lifecycle, like pregnancy, hormonal status (e.g., contraception use, menopause) can also affect blood pressure. An understanding of how different sex-specific factors affect blood pressure and risk of hypertension, a leading risk factor for heart and kidney disease as well as stroke, is urgently needed to optimize health for all persons.
For example, we and others have shown that for persons using menopausal hormone therapy, oral forms of estrogen compared to non-oral forms (e.g., transdermal, vaginal) are associated with a higher incidence of hypertension. This is an example of how sex-based factors, like menopausal status and use of hormone therapy, can influence health outcomes and must be taken into consideration into any study design to ensure the results are generalizable.
Why is the study of sex differences important not only for academics and healthcare professionals but also for the general public?
We live in a “one size fits all” society and environment which may not optimize everyone’s health and well-being. For example, the U.S. Government Accountability Office reported that 8 of 10 drugs withdrawn from the U.S. market over a four year period (1997–2000) posed greater risk to women than men, which was due to a lack of female representation in the research pipeline (cellular, animal, and human studies), leading to FDA approval.
The study of sex differences is also important in other aspects of society. For instance, crash test dummies used to determine car safety ratings are based on the male body. According to the National Automotive Sampling System–Crashworthiness Data System and Crash Investigation Sampling System, in a similar crash with similar forces on the driver, women have greater injury risk compared to men. Everything from the height of a door handle to the scale of a staircase to the size of city blocks have been designed for a 6ft-tall man. Understanding how we can make society work optimally for persons of different shapes, sizes and needs has incredible potential to benefit everyone.
In the Editorial you co-authored with Dr. Jill Becker, Editor-in-Chief of Biology of Sex Differences, you wrote: “On January 22, 2025, President Trump terminated ‘diversity, equity, and inclusion’ (DEI) discrimination in the federal workforce, and in federal contracting and spending…The executive order called ‘Defending women from gender ideology extremism and restoring biological truth to the federal government,’ indicates that the government will only ‘recognize two sexes, male and female.’ Substituting opinion for scientific fact does not make it so.” How do you foresee this policy change impacting public health and the careers of researchers in your field? In your view, how important is it to reinforce—and potentially reinstate—support for the study of sex differences in this context?
Inclusion of sex differences in all research is a critical step towards robust science that will lead to better health for everyone. Assuming that the research findings from one population are applicable to all populations has had serious ramifications. For example, most clinical drug trials have historically excluded women or have not analyzed sex-specific outcomes. However, after recognition that the sleep medication Ambien (zolpidem) was found to stay in women’s bloodstreams twice as long as in men with resulting next-day drowsiness and cognitive impairment, the FDA halved the recommended dose for women in 2013—after the drug had been on the market for years.
It is also important to recognize that while pharmacokinetics and pharmacodynamics differ by sex, these sex differences also change across the life cycle depending on age, hormonal status and co-existing chronic disease. A lack of support for research examining sex differences in health and disease will not only result in a dearth of scientists with the critical expertise across all career stages but will also ultimately hurt everyone’s health. Supporting sex differences research is a crucial step to not only prevent and treat disease, but also support well-being.
As part of our campaign, you co-authored the review titled “The Role of Sex Differences in Cardiovascular, Metabolic and Immune Functions in Health and Disease: A Review for Sex Differences in Health Awareness Day.” Could you share your insights and summarise your contribution to that review?
Overall, this review illustrates the critical nature of including incorporating sex- and gender-based factors into all aspects of cardiovascular, metabolic and immunology research. The National Academy of Medicine has outlined that “much of biomedical research still does not account for biologic differences between males and females, leading to differential success in treatments and outcomes”.
Almost a billion people around the world live with kidney disease; from my perspective, there is not only increasing recognition of the important role kidney disease plays with respect to cardiovascular morbidity and mortality with the 2023 American Heart Association Scientific Statement on the Cardiovascular-Kidney-Metabolic (CKM) syndrome, but also that an incomplete understanding of sex differences in CKM syndrome represents an important knowledge gap. The goal of our review is to highlight how an understanding of how sex-based factors across the lifespan influences pathophysiological processes leading to cardiovascular disease can result in improved health outcomes for all.
What are some of the most exciting recent developments in sex differences research that you think the public should know about?
Overall, there is increasing recognition for the potential for improved health with sex differences research across the spectrum of health conditions. There are so many examples of outstanding sex differences research and it is a challenge to highlight only a few.
Hypertension affects 1 in 3 adults worldwide and leads to stroke, heart disease, and kidney disease. Research in sex difference in blood pressure has tremendous potential to improve both quality and quantity of life, and so I will focus on this.
Recent findings on sex differences in blood pressure (BP) have direct implications for how we screen, diagnose and treat hypertension in clinical and public health settings. The discovery that women experience faster increases in BP beginning in their 30s, despite having lower BP earlier in life, suggests that current thresholds (which are largely sex-neutral) may delay diagnosis in women. Introducing sex-specific BP thresholds or age-adjusted screening guidelines could identify at-risk women earlier. Differences in how men and women respond to salt intake, sleep patterns, and BP variability point to the need for personalized interventions. Women may benefit more from addressing sleep quality and reducing BP variability. Men may need stricter sodium restrictions due to greater salt sensitivity. Since women show more pronounced effects of BP variability on brain health (e.g., risk of cerebral small vessel disease), they may need closer monitoring—not just of average BP, but of fluctuations throughout the day. Encouraging wider use of ambulatory BP monitoring (24-hour monitoring) for women, especially those with cognitive decline or stroke risk, can thus potentially improve health. Research showing that adolescents already display sex differences in nocturnal BP dipping highlights a critical window for early prevention. Developing school- or pediatric-based BP screening programs that consider sex, body composition, and sleep behaviors may reduce long-term cardiovascular risk. Public health campaigns often use one-size-fits-all messaging for hypertension, which does not account for different risk trajectories and treatment responses by sex. Creating sex-informed educational materials and public health initiatives that address women's midlife BP surge or men's early-life risks differently can improve everyone’s blood pressure and risk for stroke and cardiovascular and kidney disease.
How do you navigate the challenge of separating biological sex differences from gender-influenced behavioural or environmental factors in your research?
The goal is to be as transparent as possible in methodology and reporting of results to allow for the reader to interpret the findings in that context. For example, women with kidney failure treated with hemodialysis report lower health-related quality of life compared to men. Whether this is related to sex-specific (e.g., underdialysis due to body composition differences) or gender-specific (sociocultural) factors (e.g., greater caregiver/domestic responsibilities for women) is unknown. We aimed to determine the change in physical and mental quality of life in women and men with kidney failure 3 months after starting dialysis. We chose this primary outcome as both mental and physical health after 3 months of hemodialysis treatment have been shown to be associated with survival.
When we analyzed our results only by sex, we found that women reported greater improvements in physical but not mental health with more dialysis treatments, while men reported no difference in either domain. However, when we analyzed the data by gender score, which was independent of sex and took into account each participant’s roles and responsibilities, such as primary earner status, domestic and caregiving responsibilities, etc., we found that women who had more roles and responsibilities commonly attributed to women in a western society were more likely to report improved mental but not physical health with less dialysis. Gender score was not associated with any change in mental or physical health in men.
Recognizing that both sex and gender factors influence different aspects of our health is critical to ensuring that every person receives the treatment approach that is in alignment with their values and preferences.
What ethical considerations arise when sex differences are not taken into account in research?
Hypertension is the leading modifiable risk factor for global cardiovascular mortality in men and women. However, we found that approximately 1 in 5 antihypertensive medication studies informing hypertension guidelines used around the world do not incorporate any sex‐ and gender‐based reporting or analysis. Fewer than 1 in 4 antihypertensive medication studies have appropriate sex‐based representation in study participants, and sex‐stratified analysis of results is not common. Finally, sex‐stratified adverse events are rarely reported.
Women have a higher lifetime risk of developing Alzheimer’s disease and make up about two thirds of this patient population. However, the impact of sex on processes targeted by drugs that are in clinical trials for treatment of Alzheimer’s disease is uncertain due to limited study.
Women are about twice as likely as men to be diagnosed with major depressive disorder. Hormonal fluctuations (e.g., during menstruation, pregnancy, and menopause), along with social stressors, contribute to this disparity. Women also have higher rates of anxiety disorders, including generalized anxiety disorder (GAD), panic disorder and PTSD. However, men die by suicide at higher rates than women, despite women attempting suicide more frequently. This suggests important differences in not only sex-based biological processes and risk of developing mental health disorders but also differences in method lethality, social supports, and willingness to seek help.
A recent systematic review and meta-analysis published in BMC Psychiatry reported that female athletes reported higher rates of anxiety, depression, distress, and disordered eating, while male athletes reported more alcohol misuse, illicit drug abuse, and gambling problems. These differences underscore the importance of tailored mental health support for athletes based on sex.
How has the growing recognition of gender diversity and non-binary identities influenced your research on sex-based biological or psychological traits?
Gender is distinct from sex and is an experienced aspect of self and a social construct of norms, behaviors and roles that varies across societies and over time, which can ultimately influence a person’s biology and overall health. For example, social determinants such as gender play a significant role in shaping both the types of chemical exposures individuals encounter and the healthcare they receive afterward. For instance, if societal expectations around grooming lead both cisgender and transgender women to use more personal care products, then it is essential to prioritize the examination of substances within those products, especially those with hormonal activity. Incorporating individuals of all gender identities in exposomic research allows for a deeper understanding of how chemical exposures differ across gender groups. An example of this is how hair-straightening products containing glyoxylic acid have been associated with kidney injury.
Moreover, gender identity influences how individuals engage with not only the healthcare system but also health research. Legal frameworks and societal attitudes can significantly impact the accessibility and quality of research and medical care for intersex, transgender, and nonbinary individuals, ultimately shaping both the health outcomes and overall well-being of individuals from these communities.
How does Sex Differences in Health Awareness Day—held during National Women’s Health Week (May 12–18, 2025)—help raise awareness and improve public understanding of what sex differences truly mean? What message would you like to leave us with on this important day?
This day plays a vital role in highlighting the importance of understanding how sex (biology) and gender (sociocultural) factors influence health outcomes. This day serves as a platform to educate the public, healthcare providers, and policymakers about the ways men, women, and gender-diverse individuals may experience disease differently—from symptoms and risk factors to diagnosis, treatment response, and long-term outcomes. By drawing attention to these distinctions, the day encourages more equitable and precise healthcare approaches, promotes inclusive research practices, and challenges outdated one-size-fits-all medical models.
Recognizing sex differences in health research is about deepening our understanding so we can deliver better and more personalized health solutions for everyone. By embracing this knowledge, we move closer to a healthcare system that respects individual differences and ultimately improves lives across all communities.
Interview created, formatted, and edited by India Sapsed-Foster, Associate Publisher, with special thanks to Sofia Ahmed for her contributions and valuable insights into the significance of sex differences in health.
Follow the Topic
-
Biology of Sex Differences
This journal is unlike any other scientific journal: articles focus on sex differences in all aspects of an individual or organism. Everything from molecules to behavior and from studies of cellular function to clinical research studies are reported in this journal.

Related Collections
With Collections, you can get published faster and increase your visibility.
Sex Differences in Metabolic Regulation and End-Organ Damage
Sex differences profoundly influence endocrine and metabolic regulation, shaping disease susceptibility, progression, and therapeutic responses. This Collection aims to highlight how hormonal and metabolic interactions contribute to sex-specific pathophysiology across a range of endocrine disorders and associated systemic complications.
Research topics of interest include mechanisms and therapies addressing hormonal and metabolic dysregulation observed in conditions such as polycystic ovary syndrome (PCOS), metabolic syndrome, diabetic nephropathy, thyroid disorders, Cushing’s syndrome, and hyperaldosteronism. Emphasis is also placed on how these disorders impact multiple organ systems including the cardiovascular and renal systems, resulting in sex-specific patterns of end-organ injury and disease progression. Original research, clinical trials, translational studies, and comprehensive reviews are welcome.
Subtopics include, but are not limited to:
- Hormonal regulation of glucose and lipid metabolism by estrogens, androgens, and progesterone
- Sex-specific metabolic adaptations in obesity, diabetes, and cardiovascular disease
- Neuroendocrine and inflammatory mechanisms linking hormones to metabolic dysregulation
- Cardiovascular and renal complications of endocrine dysfunction
- Neuroendocrine control of metabolic homeostasis
- Endocrine disorders with metabolic manifestations
- Sex-based differences in drug response and therapeutic outcomes
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Nov 04, 2026
Sex Differences in Cardiovascular Disease
Sex differences play a crucial role in the development, presentation, and treatment of cardiovascular disease. Despite growing recognition of these differences, major gaps remain—particularly in understanding how biological sex and gender influence risk, diagnostics, disease mechanisms, and therapeutic outcomes. This Collection aims to address these gaps by bringing together high-quality research that advances sex-specific and gender-aware cardiovascular science.
Key areas of interest include the impact of hormonal transitions such as menopause, pregnancy-associated cardiovascular conditions, and the distinct mechanisms underlying female-predominant conditions such as HFpEF and microvascular dysfunction. Understanding these processes is essential for developing accurate risk prediction models and personalised treatment strategies.
Persistent gender disparities in diagnosis, management, and access to care also contribute to poorer outcomes—issues that remain central to achieving equitable cardiovascular health. By encouraging research across these domains, this Collection aims to support scientific progress and clinical innovation that benefit individuals of all sexes.
Possible topics include but are not limited to:
- Menopause and cardiovascular risk
- Pregnancy-associated cardiovascular disease
- Sex differences in heart failure with preserved ejection fraction (HFpEF)
- Sex differences in arrhythmias
- Microvascular dysfunction in women
- Sex-specific platelet reactivity
- Gender disparities in cardiovascular treatment
- Sex-specific cardiovascular risk prediction models
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 16, 2027




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in