Sleeping Well - A matter of timing for OSA and weight loss?
Published in Healthcare & Nursing

Obstructive Sleep Apnoea (OSA) or the intermittent obstruction of breathing during sleep, is estimated to affect one in seven adults (1 billion people worldwide) and one in two adults living with obesity also have OSA [1,2]. Obesity and OSA share a complex relationship which can make treating both challenging for an individual.
Clinical guidelines currently recommend continuous positive airway pressure (CPAP) and weight loss for OSA in those above a healthy weight. However, our current models of behaviour change suggest that whilst individuals can contemplate changing multiple behaviours at once, they can only act on one change at a time. So, does delaying the start of a weight loss intervention, whilst individuals with OSA commence CPAP, confer better OSA and weight loss outcomes?
What did we do?
Our aim was to examine whether a 6-month lifestyle intervention for people newly diagnosed with moderate to severe OSA could affect changes in weight, and whether the timing of the intervention had an impact on weight outcomes after 12 months.
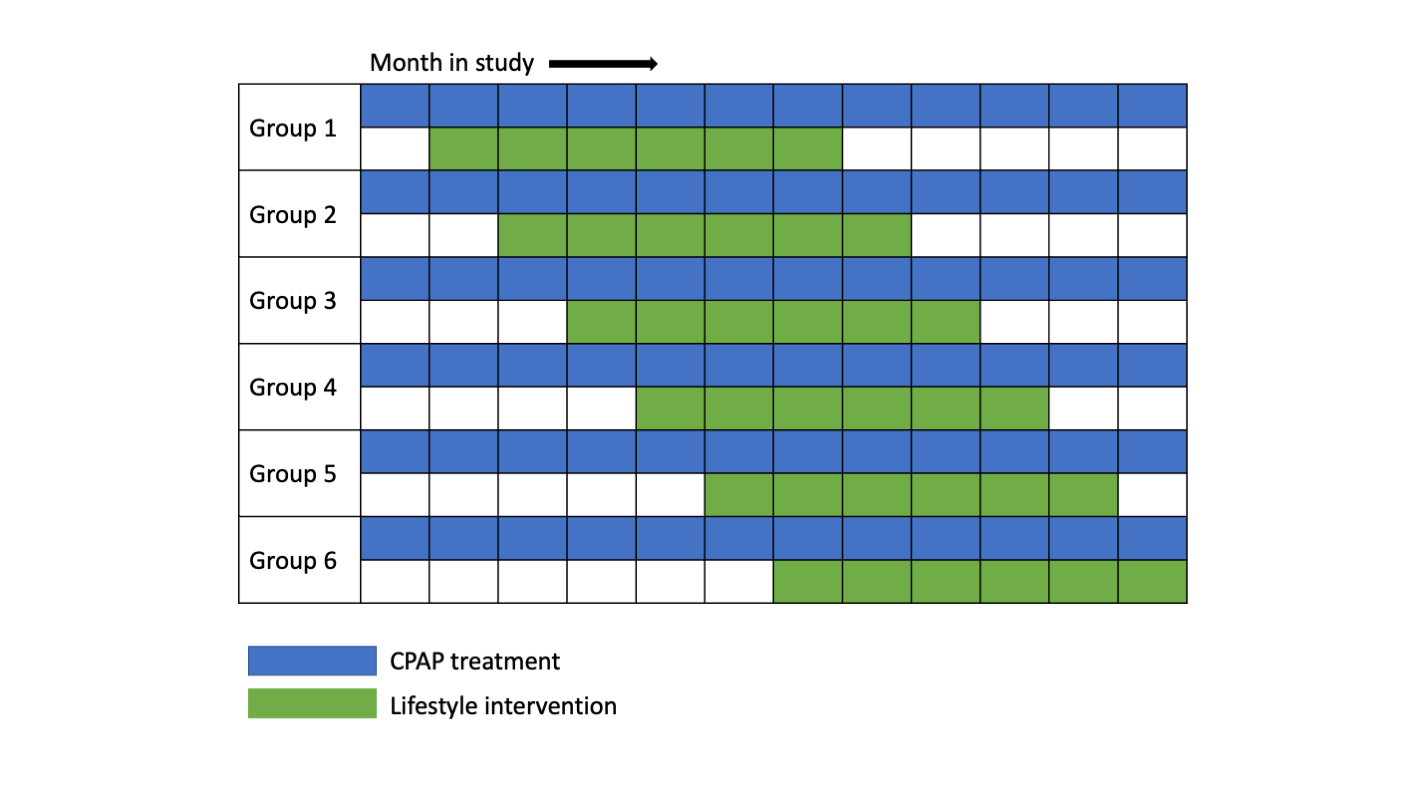
We recruited 50 participants with OSA from public hospital sleep clinics. All participants started CPAP treatment at the beginning of the trial after which they waited from 1 to 6 months before starting the lifestyle intervention.

This means the study used a stepped-wedge study design whereby every participant had 6 months in the intervention and six months out and waited at least one month before starting the intervention. Stepped wedge trials allow researchers to assess an intervention condition against a control condition without excluding anyone from care. By using different wait periods (the stepped portion of the design), we can also explore whether there was an optimum window in which to initiate a lifestyle intervention after starting CPAP treatment.
The lifestyle intervention followed a modified fasting (5:2) format whereby participants followed a reduced energy (6300-7500 kJ) intake diet for 5 days and a very-reduced (2200-2760 kJ) energy intake diet in the form of provided shakes for 2 days. Participants were also encouraged to increase physical activity.
What happened?
Timing of the lifestyle intervention had no impact on changes in weight. All groups saw a modest decrease in weight over the intervention period (6 months) and weight was significantly lower at 12 months compared to baseline for the whole group.
We also found that using CPAP alone did not lead to a significant increase in weight.
The intervention was generally well received by participants with high adherence. This may be important as it is difficult for people in the public hospital system to access this level of dietetic support for weight loss and so they valued the service highly.
Why did we do it?
Most research to date has focused on lifestyle interventions for people with mild to moderate OSA with few studies exploring the potential benefits for those with severe-OSA. As a team, we felt it most important to assess the benefits of lifestyle interventions for this, often overlooked, group. Similarly, participants were recruited from public hospitals where this level of dietetic support for lifestyle change is difficult to access yet highly valued.
Why is this important?
Behaviour change is a multi-step process that is hard to adopt and maintain. The current study suggests that for people contending with the adoption of CPAP and lifestyle change, delaying the start of lifestyle change - for however long you need (up to 6 months) will still result in positive changes and a reduction in OSA severity and weight. It appears, for this population group, there is no golden window of opportunity to start a lifestyle intervention. Start whenever you are ready.
References
- Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020 Jul;25(7):690-702.
- Drager LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstructive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. Journal of the American College of Cardiology. 2013 Aug 13;62(7):569-76.
Follow the Topic
-
European Journal of Clinical Nutrition
An international, peer-reviewed journal covering all aspects of human and clinical nutrition. This may encompass clinical, metabolic and epidemiological studies that describe nutritional interventions for clinical disease and health promotion.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in