Socioeconomic disadvantages expand the aging gap towards cognitive and socioemotional inequities
Published in Social Sciences

Marcela, a 64-year-old woman, is CEO at a publicity company. Everyday she wakes up at 8:00 AM, meditates, takes a healthy and nutritious breakfast, leaves her house at 9:30 AM, and spends 10 minutes commuting by bicycle to her office. She finishes her workday at 3:00 PM and spends the rest of the day promoting her well-being. In a peripheral rural town, Armando, same age as Marcela, daily wakes up at 4:00 AM, gets dressed, and takes a quick, high-sugar and ultra-processed breakfast before leaving his home at 5:00 AM, spends two hours traveling by public transport, and arrives at his workplace, the same publicity company, at 7:00 AM, where he cleans the bathrooms and offices until 7:00 PM. The socioeconomic differences between Marcela and Armando are clear, and it is easy to imagine the differential effect of each lifestyle on physical health. But what about the impact of socioeconomic inequality on cognitive and socioemotional processes in older adults? And why is this question critical for Latin America? In the study discussed here we reached these questions.
Socioeconomic status (SES) is a crucial trigger of economic, health, and social inequalities, and one of the most segregational factors within societies. SES describes the economic (e.g., material goods, monetary income) and social (e.g., formal education, work prestige) resources of an individual, and is a critical component of social determinants of health. The effects of SES disadvantages on physical health are widely reported, and also on cognition to some extent. Much less is known about SES impact on socioemotional processes such as emotion recognition, theory of mind (ToM; the capacity to reason about others’ mental states), and complex social emotions. While there are some clues from developmental studies, this topic has been neglected in older adults. Moreover, evidence comes exclusively from Western, Educated, Industrialized, Rich, and Democratic (WEIRD) populations, of limited relevance to understand contextual influences on brain health and dementia in older adults from upper-middle- and low‐middle‐income countries, such as those from Latin America. In this region, 54% of the national income is owned by the richest 10% of the population, and about 55% of workers are informal, making it one of the most unequal places in the world. This issue is pressing for an aging population, considering the incoming tsunami of dementia accelerated by the pandemic and its related caregiver burden across the region.
In the present study, we compared multiple cognitive and socioemotional processes among low- and high-SES healthy older adults. One of us was able to access a unique semi-rural population of Zonda, San Juan (Argentina), where poverty and natural beauty intertwine in complex scenarios. Zonda’s population is exposed to different types of vulnerability, including environmental, economic, and social factors. More than half of the young people neither study nor work. The vast majority of inhabitants perform household and farm chores. The situation worsens even more considering the recent pandemic and the high penetration of vandalism and drug sales in the area. The participants of our study (low- and high-SES older adults) were recruited from the local primary care center. We assessed and examined between-group differences in cognitive state (a set of basic cognitive functions such as attention, memory, and language), executive functions (specialized cognitive functions supporting goal-directed behavior, like flexibility and working memory), social cognition (emotion recognition and ToM), and social emotions (envy and Schadenfreude; displeasure at others’ fortune and pleasure at others’ misfortune, respectively). Then, we developed a path analysis (a statistical method that allows to examine causal relationships among several variables at once), to test a theoretically plausible model.
Relative to their high-SES counterparts, low-SES older adults showed poorer performance on all assessed domains. Critically, dysfunctions in socioemotional domains were more subtle and mediated by cognitive and executive abilities, as convergently shown by covariance and path analyses, and further corroborated by linear approaches (Figure 1). Path analysis’ results confirmed a theoretical model involving a direct effect of SES on cognitive processes, which mediated the effect of SES on socioemotional processes. Interestingly, we found different outcomes for social emotions. SES and cognition predicted an adequate experience of envy, but not Schadenfreude, in line with previous neurocognitive evidence on the differential mental demands and neural basis of each social emotion. Envy involves self-concept threat and conflict monitoring mechanisms, converging in the anterior cingulate cortex subserving executive control, which is more vulnerable to aging. Conversely, Schadenfreude is a pleasant emotion associated with reward processing in the ventral striatum, putatively implying a more basic process with less cognitive load than envy. Thus, both social emotions are differently impacted by SES in aging.
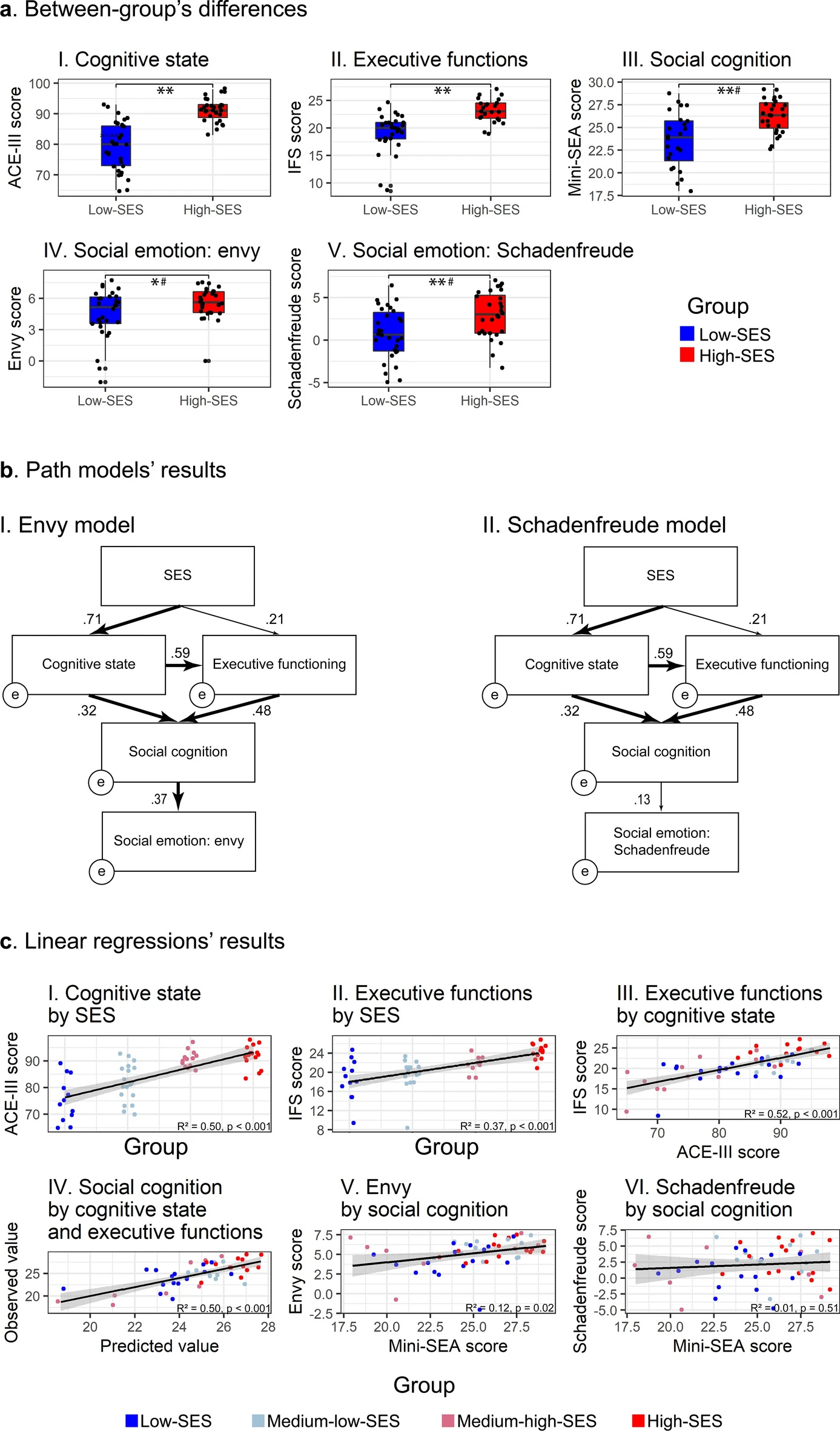
Results. (a) Data distribution and performance differences between low- and high-SES groups on cognitive state (I), executive functions (II), social cognition (III), and social emotions; envy (IV) and Schadenfreude (V). Boxplots display the median, interquartile range, and range of each variable. *p < 0.05, **p < 0.001, #p > 0.05 after controlling for depressive symptoms. (b) Path analysis models and standardized path coefficient weights for envy (I) and Schadenfreude (II) as outcome social emotions. Bold arrows depict statistically significant paths. (c) SES predicts cognitive state (I) and executive functions (II). Cognitive state predicts executive functions (III). Cognitive state and executive functions predict social cognition (IV). Social cognition predicts envy (V) but not Schadenfreude (VI). All linear regressions’ results are statistically significant (p < 0.05), except for (VI). ACE-III: Addenbrooke’s Cognitive Examination-III; IFS: INECO Frontal Screening; Mini-SEA: Mini-Social Cognition and Emotional Assessment; SES: socioeconomic status. Reproduced from https://www.nature.com/articles/s41598-022-09580-4
In conclusion, SES has a sui generis impact on cognition and an indirect impact on socioemotional processes, mediated by cognition. It seems that ‘cold’ cognitive processes are more vulnerable to unfavorable contextual factors associated with low-SES, such as diminished access to cognitively stimulating activities, education, and early life nutrition. In contrast, socioemotional processes would be more resilient to contextual adversities given its key role in helping to cope with everyday challenges through cooperation. Our results offer the first characterization of SES impact on cognitive and socioemotional processes in non-WEIRD older adults and have relevant equity-related implications for brain health. Low-SES older adults would be characterized by diminished cognitive and socioemotional abilities beyond dementia-related pathophysiological processes. Moreover, intervention programs could target cognitive impairment in order to mitigate socioemotional decline.
Putting our research in context, this study might contribute to better understand and address present and future brain health challenges in Latin America. The future of the economy will be more dependent on brain capital and human specific skills than on goods or knowledge. The region is facing an accelerated growth of the older adult population, leading to an increase in dementia incidence and associated burden of the health system. Moreover, Latin America is one of the most socioeconomically unequal regions of the world, which manifests as additional vulnerability to pathological aging. Disadvantages in SES and other inequities, such as access to the health system allowing timely diagnosis and treatment, make low-SES older adults a high-risk population. Understanding the cognitive and socioemotional dysfunction associated with low-SES in non-WIRED populations is crucial to develop global approaches to cognition and contextually situated practices to promote brain health and prevent dementia. We are still on time to improve Armando’s quality of aging and reduce the gap with Marcela’s aging conditions, but immediate efforts are needed.
Authors and Affiliations
* The figure illustrating the post has been designed and produced By Lucas Neufeld, Joaquín Migeot, Sol Fittipaldi, and Agustin Ibanez
Follow the Topic
-
Scientific Reports
An open access journal publishing original research from across all areas of the natural sciences, psychology, medicine and engineering.

Related Collections
With Collections, you can get published faster and increase your visibility.
Infectious disease diagnostics
Publishing Model: Open Access
Deadline: Sep 23, 2026
AI in Education
Publishing Model: Open Access
Deadline: Oct 09, 2026





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in