Suppression of cytokine release syndrome during CAR-T-cell therapy via an “IL-6 sponge”
Published in Bioengineering & Biotechnology

Although chimeric antigen receptor (CAR) T cells therapy has shown impressive antitumour efficacy, life-threatening complications that result from cytokine release syndrome (CRS) impose barriers to broader applications. Current IL-6 blockade strategies face many challenges: (i)The antibodies are easy to be cleared from the body. (ii) Systemic introduction of blockade antibodies generally causes some adverse toxicities such as hyperuricemia. (iii) Current CRS management strategies in the clinic need continuous monitoring of cytokines and CRS-related symptoms after CAR-T cell infusion. However, it is difficult to precisely predict whether and when a patient will develop CRS, as well as their severity level. Any delay in the administration of IL-6 blockade antibodies would result in severe toxicity including organ failure and even patient death. Even through timely intervention, permanent damage to patients could have already been caused when CRS is detected. Additionally, it would affect normal levels of IL-6 if blockade antibodies are given earlier than the onset of CRS.
Can we explore novel therapeutics that can be administered before CAR-T cell infusion to prevent CRS-related symptoms? Since we know that IL-6 contributed to several major symptoms of CAR-T induced CRS, our team believes that an ideal therapeutic for IL-6 intervention should only affect the abnormally elevated IL-6 during CRS but not interfere with normal levels of IL-6 when CRS does not exist. This approach aims to overcome the shortcomings of conventional IL-6 blockade antibodies and bypass the complex monitoring process of conventional CRS treatment strategies.
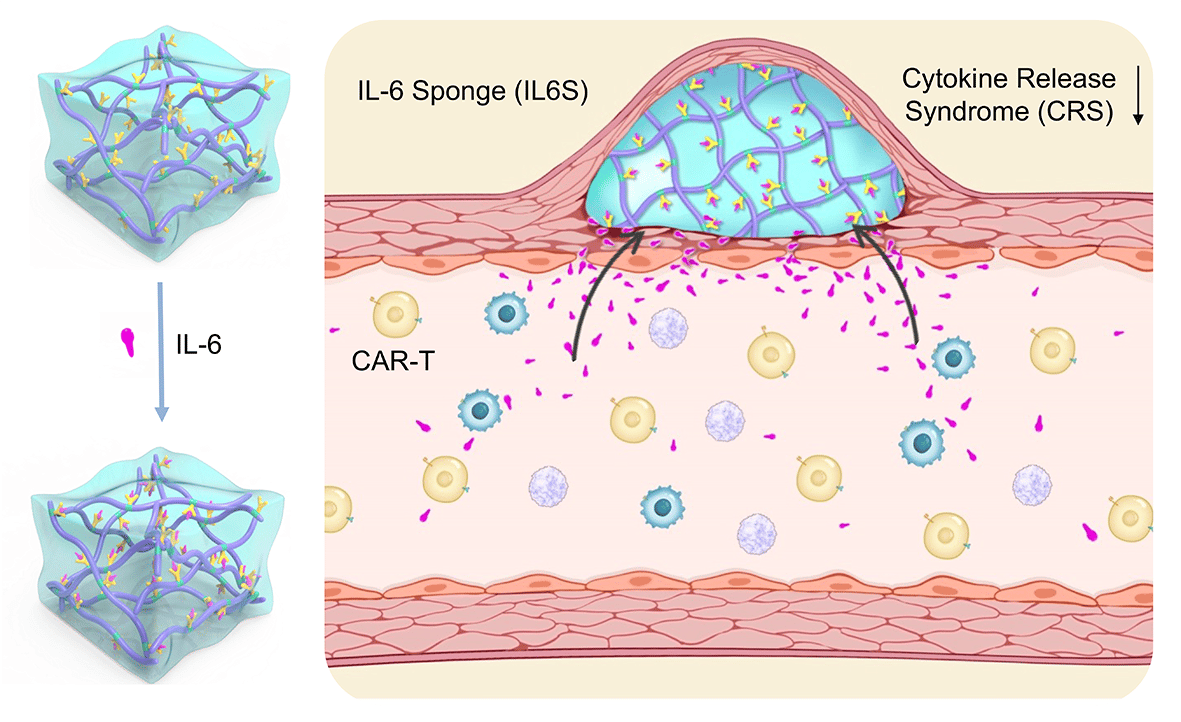
Based on the characteristics of CRS and medication challenges, we propose utilizing an IL-6 sponge (IL6S) with IL-6-specific antibody chemically conjugated to a thermo-sensitive hydrogel to prevent CAR-T cell-induced CRS (Fig. 1). By adjusting the antibody concentration in the hydrogel, the IL-6 adsorption threshold of IL6S can be precisely controlled. The optimized IL6S does not affect IL-6 levels under normal conditions or when CRS does not occur. IL6S can be administered prior to CAR-T cell infusion to capture any abnormally increased IL-6 in a real-time manner when CRS occurs, thus avoiding the complex CRS monitoring process.
Although the therapeutic effect of IL6S was quickly verified in a CRS-mimicking model, it is a huge challenge to establish a real CAR-T cell-induced CRS model. To address this issue, our team sought a collaboration with Prof. Tongcun Zhang’ lab at Wuhan University of Science and Technology, and Prof. Xingxu Huang’s team at ShanghaiTech University, both of the teams are experienced in CAR-T cell fabrication and animal model construction. With their great support, we successfully built CAR-T induced CRS models in humanized immune system mice. With respect to the administration of free IL-6 antibodies, the subcutaneously administrated IL6S largely suppressed CAR-T-cell-induced CRS, substantially improving the animals’ survival and alleviating their levels of fever, hypotension and weight loss, as well as maintaining antitumour efficacy of CAR-T cells in vivo. Another advantage of IL6S is its ease of removal from the injection site with a syringe following an ice coating-induced gel-sol transition. This convenient process allows for the removal of both the IL6S material and the adsorbed IL-6.
Our team highly appreciates the insightful comments provided by the editor and reviewers, which have significantly improved the quality of our manuscript. For instance, one key aspect that required consideration was the dosage required when utilizing the IL-6-adsorbing hydrogel to prevent CRS in patients. We calculated that for grade 1, 2, 3, and 4 CRS, IL6S volumes of approximately 0.44, 2.20, 7.76, and 11.04 mL respectively would be sufficient to fully adsorb the abnormally elevated IL-6 in human patients. Moreover, multi-site injections could be employed for clinical translation, ensuring that the volume at each injection site remains small. Another potential solution for clinical translation involves using an ex vivo dialysis device, similar to haemodialysis used in clinical settings. In this approach, IL6S can be coated or fixed on the walls of the dialysis pipe. As the patient’s serum passes through the dialysis unit, the abnormal elevated IL-6 can be effectively captured by IL6S. This method also offers the advantage of easy removal of IL6S after addressing CRS.
This research spanned five years from its beginning to the acceptance of the article. Although the journey was long and challenging, we take immense pride that our research provides the field a novel method for the management of CAR-T cell-induced CRS. Our results could facilitate a shift in CRS management, from complicated monitoring to proactive prevention. Given that CRS with similar characteristics also occurs in a portion of SARS-CoV-2-infected COVID-19 patients, IL6S holds the potential to be employed to preventively control relevant symptoms during antiviral therapy.
Follow the Topic
-
Nature Biomedical Engineering
This journal aspires to become the most prominent publishing venue in biomedical engineering by bringing together the most important advances in the discipline, enhancing their visibility, and providing overviews of the state of the art in each field.

Related Collections
With Collections, you can get published faster and increase your visibility.
Implantable wireless communication technologies
Publishing Model: Hybrid
Deadline: Nov 28, 2026
Medical Ultrasound: Emerging Techniques and Applications
Publishing Model: Hybrid
Deadline: Jan 29, 2027




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in