Surviving a Pandemic Without a Local Health Department
Published in Public Health

As schools, businesses, travel, and life as we knew it began to shut down in March of 2020, an often repeated phrase was “listen to your local health official.” Federal officials encouraged the public to tune into local leaders who could provide detailed accounts of what was happening in their local communities – how many new cases were there, how many people were hospitalized, how many ventilators were available, and how many people were dead (or dying). Similarly, as the country began to reopen during the summer of 2020, the public once again was told to “listen to your local health official” for instructions regarding how to safely navigate the world still swarming with COVID.
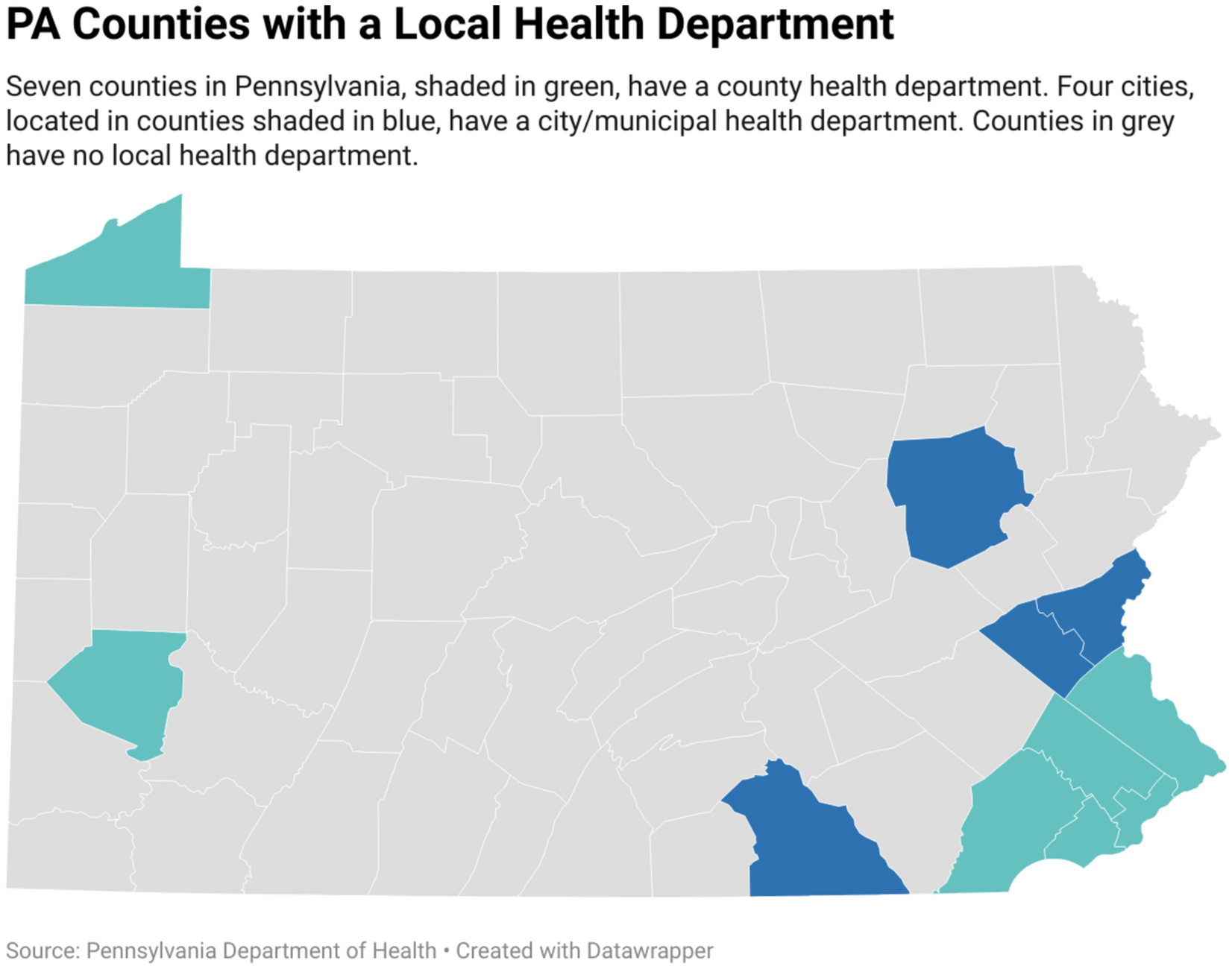
For those of us living in the 56 counties of Pennsylvania where there is no health department, these instructions to “listen to your local health official” made no sense. There was/is no local health official. There were local health clinics (staffed with nurses; not trained in public health) and public health professionals in Harrisburg, nearly 5 hours away, who were directing the public health response to the pandemic, but nothing about that felt relevant or local.
We were required to survive the pandemic without a local health official to listen to or lead us.
In Crawford County, home to Allegheny College and the research team that completed this study, a group of volunteers – a county commissioner, epidemiology professor, and retired science teacher – banded together to track cases, answer community questions, and establish a single online resource page (on Facebook because there was no money, resources, or expertise to build out a county health website). This band of volunteers had little (if any) contact with leaders in Harrisburg, but they shared information within the county and did their best to keep community members informed and calm through the initial crisis of the pandemic.
From 2020-2022 – we felt the void left by not having a local health department as a pandemic turned our worlds upside down. We had to source our own COVID tests, set up a contact tracing protocol (with only one individual in the community trained in public health), track our own data, establish relationships, and follow policies set by leaders who had never stepped foot in our community and who we did not know or trust.
It was not public health practice; it was survival.
In the years following, our research team started to ask questions that went beyond the pandemic – are counties with local health departments healthier? Do residents there have access to better healthcare? Do they get vaccinated more often?
These questions led to us completing an ecological epidemiological study where we assessed community health impacts, including obesity, infant mortality, smoking and vaping, percent of the population with health insurance, and youth suicidality, among others comparing counties with and without a local health department. We found that overall the counties in Pennsylvania without a local health department had poorer health outcomes compared to counties with a local health department after controlling for race, education, income, access to health insurance, and the urban–rural status of each county.
We believe there are significant benefits to having a local health department, and more than half of the population in Pennsylvania does not have access to those benefits due to the public health governance structure in the state. Policy changes are needed in Pennsylvania to establish and maintain a local health department in every community. Local health departments provide the foundation for creating healthy communties and they are needed throughout the state of Pennsylvania; not just in 11 of 67 counties.
Follow the Topic
-
Discover Public Health
This is an open access journal publishing research from all fields relevant to public health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Digital Frontiers in Public Health: Data-driven Solutions and Technologies for Efficiency, Effectiveness, and Equity
In recent years, the landscape of public health has been transformed by unprecedented access to high-quality data, advances in data storage and processing, and a growing willingness to share information across jurisdictions. The global response to the COVID-19 pandemic exemplified how coordinated data use and technological innovation can accelerate decision-making, enhance surveillance, and save lives. These developments mark a new era in which the application of modern data analytics in evidence-driven public health practices is not only possible but essential.
Building on this momentum, contemporary innovations are contributing to significant improvements in the three Es of public health: efficiency, effectiveness, and equity. Improved efficiency enables resources to be allocated and managed in a manner that generates the maximum attainable outputs; enhanced effectiveness ensures that public health policies, interventions, and practices achieve the expected health outcomes; and strengthened equity promotes fair access to healthcare and public health services across all populations. Together, these dimensions reflect the evolving priorities and capabilities of modern public health systems.
This Collection, “Digital Frontiers in Public Health: Data-driven Solutions and Technologies for Efficiency, Effectiveness, and Equity,” invites contributions that explore these themes through empirical studies, methodological advancements, case studies, and policy analyses. We seek manuscripts that highlight innovative data applications, cross-sector collaborations, digital health initiatives, and strategies that enhance equity through technology and data integration, as well as collaborative public health practices.
Topics of interest include, but are not limited to:
- Applications of novel data linkage and analytics methods in public health
- The role of participation and co-creation in addressing public health issues
- Digital and technological innovations in public health
- Complete or partial assessments of triple Es in public health
- Economic evaluations of public health interventions
By showcasing diverse approaches from around the world, this Collection aims to provide a comprehensive overview of how data-driven innovations are reshaping public health practice today, and in the future. Researchers, practitioners, and policymakers are encouraged to share their insights and experiences to contribute to this critical dialogue on the future of public health.
This Collection supports and amplifies research related to SDG 3.
Keywords: digital applications; data sharing; data infrastructure; economic evaluations; health equity; public health; policy analysis; health informatics
Publishing Model: Open Access
Deadline: Sep 30, 2026
Pediatric Noncommunicable Diseases: Policy, Practice, and Public Health
Non-Communicable Diseases (NCDs) such as diabetes, asthma, congenital heart conditions, and childhood cancers are increasingly recognized as significant contributors to morbidity and mortality among children and adolescents. Despite their growing impact, pediatric NCDs are often underrepresented in health policies and global health agendas, which traditionally focus on infectious diseases or adult populations.
According to the World Health Organization (WHO) and UNICEF, NCDs are responsible for approximately 20% of all deaths among adolescents aged 10–19 globally. Moreover, over 50% of disability-adjusted life years (DALYs) in this age group are attributed to NCDs, with mental health conditions such as depression, anxiety, and conduct disorders being the leading contributors. The burden is not only medical but also social and economic. Children with chronic conditions often face stigma, reduced educational opportunities, and long-term health complications. Additionally, 70% of premature adult deaths from NCDs are linked to behaviors that begin in childhood and adolescence, such as poor diet, physical inactivity, and exposure to tobacco and alcohol.
Despite this, pediatric NCDs remain under-prioritized in global health strategies. Addressing them requires a life-course approach that includes early prevention, integrated care, and supportive environments. Strengthening health systems to respond to pediatric NCDs is essential for achieving universal health coverage and sustainable development goals.
This Collection supports and amplifies research related to SDG 3.
Keywords: Pediatric Non-Communicable Diseases, Child and Adolescent Health, Chronic Illness in Children, Mental Health, Early-Life Risk Factors, Global Health and NCDs
Publishing Model: Open Access
Deadline: Jul 31, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in