The EGR3 regulome of infant KMT2A-r acute lymphoblastic leukemia identifies differential expression of B-lineage genes predictive for outcome
Published in Cancer
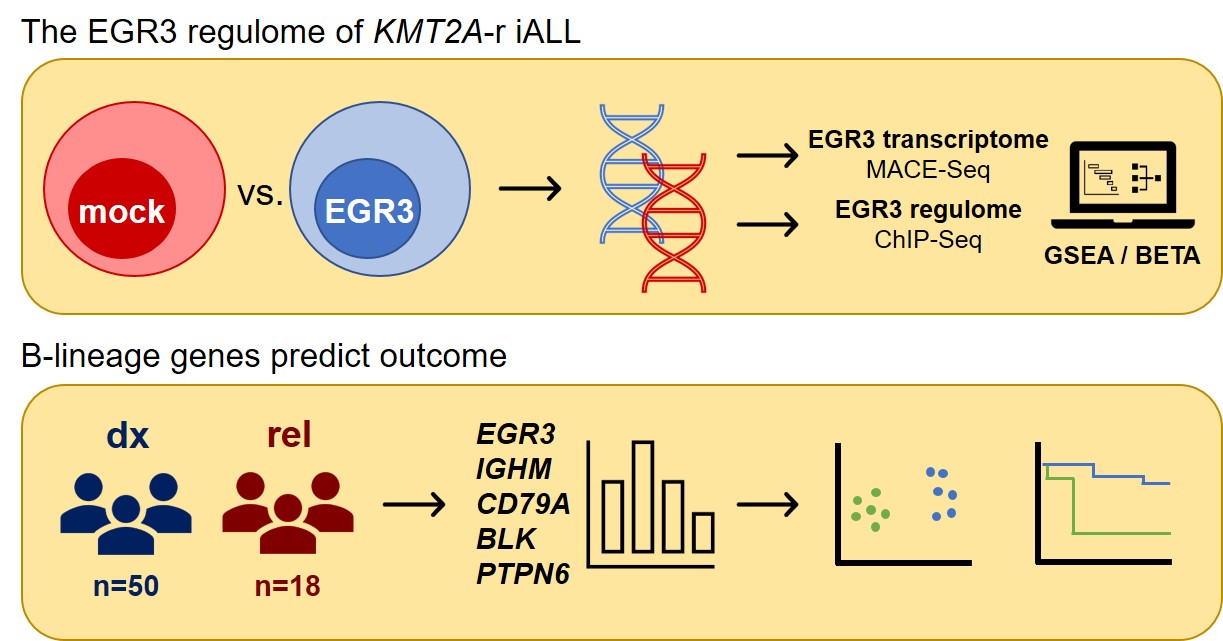

Infant acute lymphoblastic leukemia (iALL) is a devastating disease which mainly arises due to the occurrence of oncogenic KMT2A-rearrangements (KMT2A-r). Most patients suffer from rapid development of chemo-resistance and subsequent on-treatment relapse, associated with high mortality (1–4). We previously reported approximately 100-fold increased expression levels of the transcription factor-encoding gene EGR3 at relapse compared to primary diagnosis (5). This prompted us to investigate the transcriptional network of EGR3 in the context of KMT2A::AFF1 iALL, referred to as the EGR3 regulome.
The establishment of an EGR3-overexpressing cell culture model using the KMT2A::AFF1 cell line SEM enabled characterization of the EGR3 transcriptome via MACE-Sequencing followed by differential gene expression analysis. Gene set enrichment analysis demonstrated ‘B cell receptor signaling’ to be the highest ranked gene set. This was the first hint that EGR3 might be related to B lineage commitment. To further elucidate this, flow cytometry was performed to analyze the phenotype of our cell culture model in comparison to an empty vector control SEM cell line. This clearly demonstrated EGR3-related expansion of phenotypic B cells indicated by strong upregulation of CD19 positivity and occurrence of a CD19high CD79A+ population.
ChIP-Sequencing was used to analyze directly EGR3-regulated target genes. To integrate ChIP- and MACE-Sequencing data sets, a binding and expression target analysis was applied. This showed that EGR3 acts as a direct regulator of many B lineage marker genes, i.e. CD19, BLK, CD79A, PTPN6, and CD22. We performed motif scanning of upregulated but not direct targets of EGR3 to identify collaborating transcription factors. Thereby, we observed enrichment of the PAX5 binding motif, suggesting cooperation of EGR3 and PAX5 in a transcriptional network mediating B lineage specification and commitment.
A verification of these results was possible through gene expression analysis of a cohort of 50 KMT2A::AFF1 iALL patient samples from primary diagnosis. Pearson correlation testing revealed transcriptional co-dependencies of EGR3, IGHM and BLK. Interestingly, the tested B lineage marker genes IGHM, CD79A, BLK and PTPN6 correlated strongly and highly significant with each other, suggesting their collective belonging to a distinct transcriptional program. This became corroborated by a principal component analysis uncovering a strictly dichotomous clustering of patients. We therefore concluded that patients can be clearly separated depending on the expression of only four B lineage commitment genes. That this observation has a clinical impact became clear when we performed an event-free survival analysis of patients assigned to the observed groups: Those patients with absent B lineage gene expression demonstrated a significantly inferior long term event free survival than patients with high B lineage gene expression. This result was not affected by patient age, white blood count or HOXA status as possible confounders.
Investigation of 18 KMT2A-r iALL patients at time of relapse showed that bimodal distribution of patients was sustained at relapse, while EGR3 expression was uncoupled from expression of B lineage marker genes. We therefore assume the elevated EGR3 expression at relapse to be rather reflective of inflammatory conditions than being indicative for B lineage commitment as it is the case at primary diagnosis.
Moreover, we can only speculate whether the identified subgroups indicate different levels of maturity and distinct differentiation stages, i.e. early and late pro-B cells. One could also argue that in the inferior EFS group, a more aberrant oncogenic signaling interferes with B lineage signaling pathways mimicking a less differentiated cell identity on the transcriptional level.
Importantly, our observations suggest eligibility of the four B lineage marker genes IGHM, CD79A, PTPN6, and BLK for gene expression-based risk stratification. The latter is an indispensable pre-treatment step assigning patients to appropriate intervention groups to avoid overtreatment of low risk, and undertreatment of high risk patients. In this context commonly applied high risk factors are KMT2A-r, age at diagnosis below 6 months, high white blood count, poor glucocorticoid response and occurrence of CNS leukemia (2,6,7). Based on our results, we report that patients at high risk can be further subclassified depending on expression of B lineage specification genes. This adds a new set of predictive risk markers to the clinician’s toolbox and will hopefully improve stratification of high risk patients, thereby supporting clinical decision making.
In summary, our study identified EGR3 as a mediator of B lineage specification and commitment in infant KMT2A::AFF1 ALL and characterized the EGR3 regulome in detail. Furthermore, we present four B lineage markers whose gene expression can be applied for substratification of patients at high risk.
References
- Pieters R, Schrappe M, De Lorenzo P, Hann I, De Rossi G, Felice M, et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (Interfant-99): an observational study and a multicentre randomised trial. Lancet Lond Engl. 2007 Jul 21;370(9583):240–50.
- Pieters R, De Lorenzo P, Ancliffe P, Aversa LA, Brethon B, Biondi A, et al. Outcome of Infants Younger Than 1 Year With Acute Lymphoblastic Leukemia Treated With the Interfant-06 Protocol: Results From an International Phase III Randomized Study. J Clin Oncol. 2019 Sep;37(25):2246–56.
- Meyer C, Burmeister T, Gröger D, Tsaur G, Fechina L, Renneville A, et al. The MLL recombinome of acute leukemias in 2017. Leukemia. 2018 Feb;32(2):273–84.
- Driessen EMC, de Lorenzo P, Campbell M, Felice M, Ferster A, Hann I, et al. Outcome of relapsed infant acute lymphoblastic leukemia treated on the interfant-99 protocol. Leukemia. 2016 May;30(5):1184–7.
- Külp M, Siemund AL, Larghero P, Dietz A, Alten J, Cario G, et al. The immune checkpoint ICOSLG is a relapse-predicting biomarker and therapeutic target in infant t(4;11) acute lymphoblastic leukemia. iScience. 2022 Jul 15;25(7):104613.
- Salzer WL, Jones TL, Devidas M, Dreyer ZE, Gore L, Winick NJ, et al. Decreased induction morbidity and mortality following modification to induction therapy in infants with acute lymphoblastic leukemia enrolled on AALL0631: a report from the Children’s Oncology Group. Pediatr Blood Cancer. 2015 Mar;62(3):414–8.
- Tomizawa D, Miyamura T, Imamura T, Watanabe T, Moriya Saito A, Ogawa A, et al. A risk-stratified therapy for infants with acute lymphoblastic leukemia: a report from the JPLSG MLL-10 trial. Blood. 2020 Oct 15;136(16):1813–23.
Follow the Topic
-
Leukemia
This journal publishes high quality, peer reviewed research that covers all aspects of the research and treatment of leukemia and allied diseases. Topics of interest include oncogenes, growth factors, stem cells, leukemia genomics, cell cycle, signal transduction and molecular targets for therapy.


![When PSMA-targeted therapy is not enough: high-risk localized prostate cancer after repeated [177Lu]Lu-PSMA radioligand therapy](/cdn-cgi/image/metadata=copyright,fit=scale-down,format=auto,quality=95,width=256,height=256/https://public-storage.zapnito.com/Ku6h7Yyp4Q0LXqRRMICCHR2v4LcOsmxMrmDPtOYuI1c)



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in