Thiamine responsive high output heart failure of adults: an under-recognized entity
Published in Healthcare & Nursing
Nowadays beriberi caused by thiamine deficiency is rare in healthy individuals in food-secure settings. Classically described as dry and wet beriberi, the condition is fraught with
potentially multiple serious manifestations involving multiple organ systems in the body.
Cases of thiamine deficiency as part of pan-nutrient deficiency have been reported in
populations with famines, war-torn areas from conflict-ridden zones etc. besides scattered
reports in alcoholics and post-bariatric surgery subjects. The absence of validated
diagnostic criteria, lack of thiamine testing, and conservatism in diagnosis may explain
scant reporting and inadequate descriptions of beriberi. Accordingly, the manifestations are
forgotten and recent literature about these is insufficient. More importantly thiamine deficiency
may get exaggerated in various clinical conditions generating high metabolic demands like
pregnancy, fever, sepsis, recurrent vomiting etc. on one hand and many of these clinical
manifestations may mask underlying thiamine deficiency.
The background of the study titled “Thiamine responsive high output heart failure of
adults: an under-recognized entity” was a persistent observation of reports of thiamine
deficiency presenting as nonalcoholic Wernicke’s encephalopathy, polyneuropathy in
peripartum women, an encephalitic form of dry beriberi, pulmonary hypertension and lactic
acidosis as infantile beriberi, and thiamine-responsive GI upset as the first description of
possible gastric beriberi. Coupled with these descriptions we observed several cases of
heart failure of unknown etiology that respond to thiamine administration.
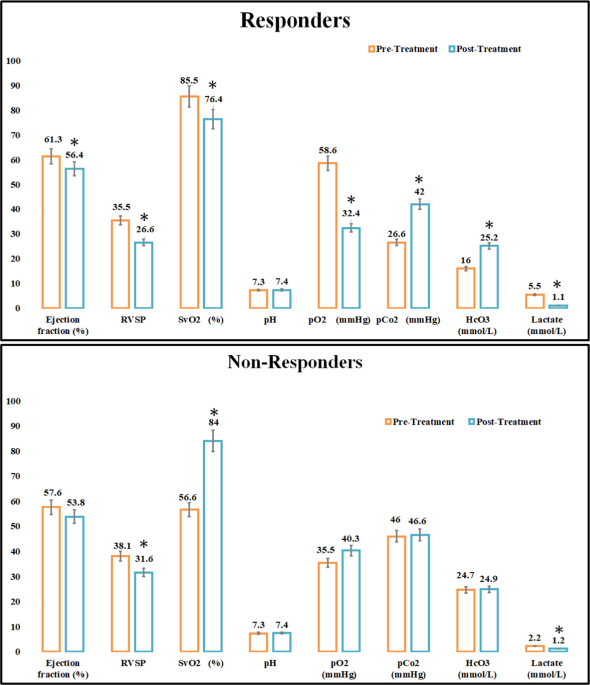
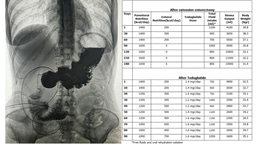
Therefore in this study patients presenting with features of high-output heart failure (HOHF) were evaluated and treated with intravenous thiamine 600 mg thiamine I.V. infusion in normal saline once a day for 3 to 5 days, followed by oral tablets of 100 mg per day for 21 days after discharge from the hospital) and the response to thiamine was monitored over 2, 24 and
72 h (lactate response was monitored within 2 h, the clinical and biochemical response
was observed in 24 h and a complete clinical response was observed in 72h). Thiamine deficiency was seen as a common phenomenon in heart failure, but cases of beriberi-related HOHF, which responded to thiamine alone were in younger adults with no co-morbidities or underlying heart disease. Responders showed considerably lower mean thiamine pyrophosphate levels and higher mean lactate and venous oxygen saturation than non-responders. Notably, the mean drop in lactate and SVO2 following thiamine therapy was more in responders.
We conclude that in the areas having a high prevalence of thiamine deficiency and in absence of thiamine testing patients having features of high output state, high blood lactate levels, higher venous oxygen saturation, normal QRS duration and sinus tachycardia on ECG
should be given a thiamine challenge. The drop in 2-h lactate was accompanied by a drop in
venous oxygen saturation may suggest beriberi as a cause of HOHF. In addition, the
temporal association of axonal neuropathy with these features of HOHF makes the
diagnosis more likely. Well-designed randomized controlled trials on larger samples are
required to confirm our preliminary findings.
Follow the Topic
-
European Journal of Clinical Nutrition
An international, peer-reviewed journal covering all aspects of human and clinical nutrition. This may encompass clinical, metabolic and epidemiological studies that describe nutritional interventions for clinical disease and health promotion.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in