Why we studied diabetes screening uptake in Aceh, Indonesia
Published in Healthcare & Nursing, Social Sciences, and General & Internal Medicine


The story behind the research

When we started our research project in 2019, the ambition of Indonesia’s health system was clear: free, community-based screening services for noncommunicable diseases (NCDs) such as hypertension and diabetes were rolled out broadly — every community health center (“Puskesmas”) and many village level “Posbindu” (health posts) offered screening. Yet, uptake remained surprisingly low.
We began asking: why? If the financial and logistical barriers are largely addressed (i.e. screenings are free and local), what holds people back from actually going? Are there knowledge gaps? Misconceptions? Attitudes that deter action? And how much does socioeconomic status or education play a role in who gets screened?
Our aim was to probe these barriers, from the perspective of the individuals—their knowledge, beliefs, and behaviors (KAP)—in a representative sample of adults aged 40–70 who should be screened per WHO PEN guidelines but who had not been recently screened. We believed that a deeper understanding of these “demand-side” obstacles could inform better strategies to close the gap in screening uptake, beyond just increasing supply.
Our approach
To explore these questions, we conducted a cross-sectional, population-based survey across the Indonesian province of Aceh in our paper "Hypertension and diabetes screening uptake in adults aged 40–70 in Indonesia: a knowledge, attitudes, and practices study". Using a two-stage cluster random sampling design, we selected 152 villages to capture a mix of urban and rural contexts and recruited adults aged 40 to 70 years — the target group for hypertension and diabetes screening under national guidelines. The study ultimately included 2,080 respondents, providing one of the largest datasets to date on community-level NCD screening behavior in Indonesia.
Data were collected through structured face-to-face interviews led by trained local enumerators. The questionnaire, adapted from WHO’s STEPS framework and national health surveys, captured four domains:
- Sociodemographic characteristics (e.g., education, income, residence);
- Knowledge of hypertension and diabetes risk factors and screening needs;
- Attitudes toward preventive screening and perceived personal risk; and
- Practices related to past screening experiences and health-seeking behaviors.
What stood out to us most
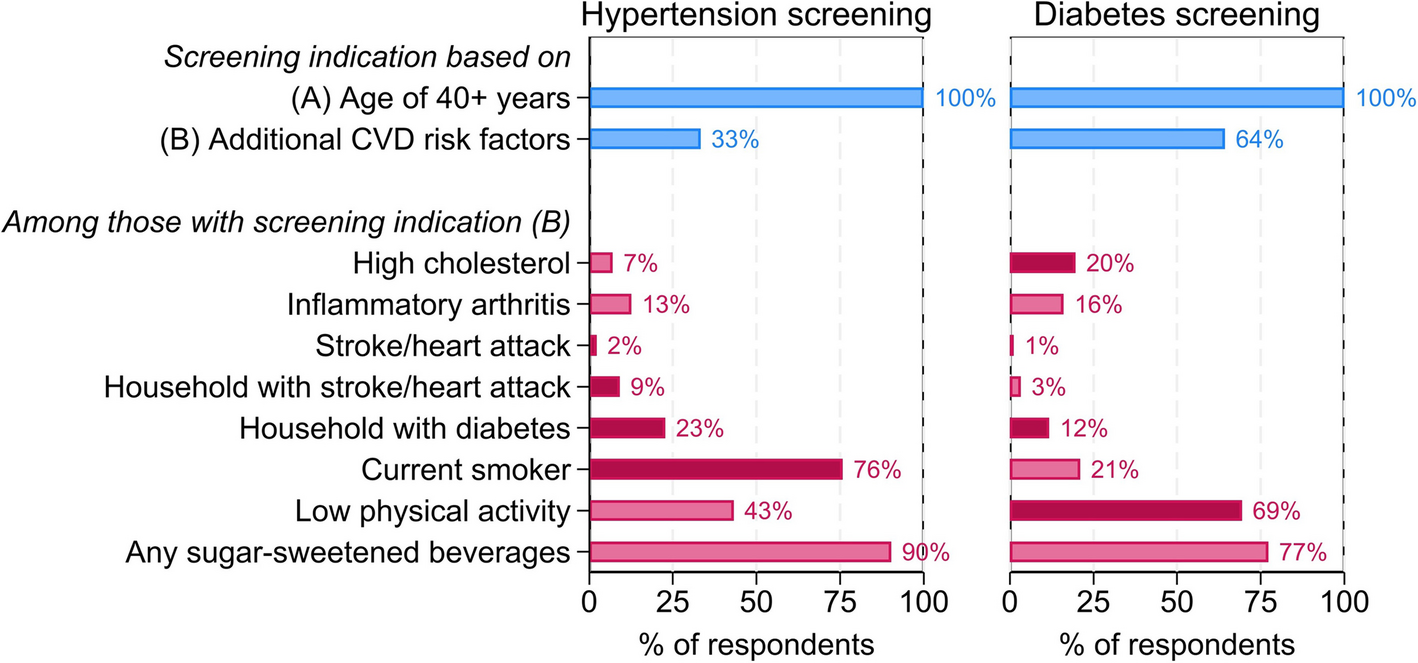
One of the most striking findings was that about 41% of respondents had never had any blood pressure or glucose check—despite free, local screening availability. Whenever respondents had been screened before, blood pressure checks were far more common than glucose checks: nearly everybody had a blood pressure measurement, but only ~21% had a blood glucose check in their last screening. That suggests that hypertension screening may be more opportunistically integrated into health encounters. In contrast, glucose testing often requires more resources, lab support, or is treated as a conditional add-on, not standard care.
We found critical gaps in the understanding of diabetes and hypertension: while most respondents were aware of these conditions, many did not know about which lifestyles may lead to diabetes and hypertension nor that they can start off ‘silently’ – without any symptoms. Instead, it was commonly believed that only those feeling ill should undergo screening.
We also saw clear socioeconomic gradients: living in rural areas, having lower education, and being in lower wealth quintiles were all strongly associated with lower knowledge and lower screening uptake. It reinforced our belief that universal access alone is not sufficient; equity in health demands addressing awareness, beliefs, and social determinants.
What this means going forward
From our work, several actionable lessons emerge:
-
Make screening guidelines and risk messaging more salient
Many people don’t see screening as relevant unless symptoms arise. Health education campaigns need to stress that hypertension and diabetes can be “silent” and that people without symptoms should still be screened. -
Differentiate strategies for hypertension vs. diabetes
The barriers appear disease‐specific—blood pressure measurements seem more normalized in care contexts, while glucose testing is rarely routine. Tailored strategies may be needed for each, including that health systems could equip more frontline facilities with affordable point-of-care glucose devices and protocols. -
Leverage trusted community platforms
Posbindu screening posts were underutilized (only 9% of last screenings) despite being very local. Strengthening their visibility, reducing resource constraints, and reframing usage so people don’t dismiss them as for “the elderly only” could help. -
Target disadvantaged groups with additional support
Lower-educated, rural, and lower-wealth individuals lag in both knowledge and uptake. Interventions (e.g. community outreach, peer education, mobile reminders) should especially prioritize those groups.
We hope our work helps health planners in Indonesia — and other settings with persistent gaps in NCD screening — in their efforts to holistically bridge the last mile: not just offering services, but ensuring they are seen, understood, trusted, and accessible by everyone. While there are some evidence-based approaches on how to achieve this (also see our paper on the effect of SMS reminders on diabetes and hypertension screening uptake in the same study population), more large-scale, effective, and innovative ideas are needed to ensure NCD care for all!
Follow the Topic
-
BMC Global and Public Health
An open access, transparent peer review journal publishing outstanding and influential research and opinion of broad interest to all professional communities involved in global and public health research, policy-making, implementation and delivery worldwide.

Related Collections
With Collections, you can get published faster and increase your visibility.
Advanced data-driven analytical frameworks to support and improve policy decisions
BMC Global and Public Health is calling for submissions to our Collection on how the integration of advanced data-driven methods in public health policy is rapidly transforming how we understand and respond to global health challenges. This Collection focuses on the application of innovative statistical modelling, machine learning, and geographic information systems (GIS) to inform health policy decisions. By integrating data from surveys and health records with information on social and environmental determinants, researchers can uncover actionable insights that enhance the effectiveness and efficiency of health interventions across diverse populations.
The relevance of these advanced methodologies is underscored by recent advancements in methods for data collection and analysis, which have enabled researchers to create more precise models for predicting disease outbreaks, evaluating health interventions, and addressing health disparities. As public health continues to confront complex issues such as pandemics and non-communicable diseases, the ability to leverage data-driven strategies becomes increasingly vital for crafting evidence-based policies that are responsive to real-world challenges.
Continued research in this area could lead to groundbreaking methodologies that enhance our understanding of health dynamics and improve public health responses. Future advancements may include the development of real-time data analytics for tracking disease spread, enhanced spatial epidemiological models that account for environmental variables, and improved collaboration between data scientists and public health professionals. By further integrating data science with public health, we can pave the way for more effective interventions and ultimately improve health outcomes globally.
We encourage submissions in the following areas, with a particular interest in studies relevant to low- and middle-income countries (LMICs); however, contributions from all settings are welcome, including:
- Applications of Machine Learning in Public Health
- Spatial Epidemiology and Disease Mapping
- Statistical Modeling for Health Policy Decisions
- GIS in Public Health Decision Making
- Evidence-Based Approaches to Infectious and Non-communicable Diseases
This Collection supports and amplifies research related to SDG 3: Good Health and Well-being.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Nov 14, 2026
Strategies for reducing cross-border health challenges
BMC Global and Public Health is calling for submissions to our Collection on strategies for reducing cross-border health challenges. This Collection aims to address the pressing need for innovative, collaborative solutions to health issues that transcend national boundaries, such as infectious disease outbreaks, migration-related health disparities, and the global impact of climate change on health systems.
The aim of this Collection is to explore the multifaceted nature of cross-border health challenges and to identify actionable strategies that promote health equity and resilience. Potential topics include the role of international partnerships, data sharing, and policy harmonization in managing health crises. Submissions addressing technological innovations, public health interventions, or socio-political frameworks to tackle these global issues are highly encouraged.
Our goal is to foster a deeper understanding of how interconnected health systems and collaborative actions can reduce the burden of cross-border health challenges. We invite submissions on the following subtopics:
Strengthening health system resilience in response to transnational disease outbreaks.
Addressing health disparities among migrant and refugee populations.
The impact of climate change on cross-border health challenges.
Leveraging technology and big data to enhance global health surveillance and response.
Policy frameworks for improving international health collaboration.
Case studies of successful cross-border public health initiatives.
By focusing on scalable and sustainable solutions, this Collection seeks to advance knowledge and inform practice in tackling health challenges that require coordinated global action.
We encourage work from local, regional, national, and global partnerships and collaboration among multidisciplinary scientists using multiple methodologies. We ask that authors be careful to use non-stigmatizing/preferred language in their manuscripts as outlined in relevant language guidelines for their respective fields.
This Collection supports and amplifies research related to SDG 3: Good Health and Well-being, SDG 5: Gender Equality, and SDG 10: Reduced Inequalities.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer-review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Sep 29, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in