Challenging the gold standard: Transdiagnostic cognitive behavioural therapy is just as effective as disorder-specific therapy
Published in Behavioural Sciences & Psychology
In an ideal world, diagnostic categories for mental disorders are narrow and distinct: patients with social anxiety are mainly concerned with a fear of social rejection; patients with panic disorder are mainly concerned with a fear of their physical symptoms. The gold standard mental health treatment focuses on the specifics of a particular disorder. It assumes that different disorders emerge through distinguishable mechanisms and should therefore be treated using specialized methods. While diagnostic categories are useful, they are essentially man-made and disguise evident comorbidity between different disorders. In the real world, co-occurring mental disorders are the norm, not the exception. Transdiagnostic psychotherapy provides a treatment that is applicable across different disorders by focusing on shared underlying mechanisms. Recent trials have focused particularly on unified transdiagnostic cognitive behavioural therapy (TD-CBT), in which a standard set of modules is applied in the same sequence to all patients, irrespective of their diagnosis. Can such a “broadband” approach address shared commonalities across disorders at once? The short answer of our meta-analysis is yes! In the following, I will share more about our study, including a glimpse behind the scenes.
The effectiveness of TD-CBT has been evaluated in randomised controlled trials (RCTs) with meta-analytic evidence supporting the approach. However, there are three limitations that have motivated our meta-analysis. First, most previous syntheses focus only on a specific disorder or setting (e.g., face-to-face treatments in anxiety disorders). Second, results on the comparability of unified TD-CBT and disorder-specific CBT (DS-CBT) are conflicting. And finally, the most comprehensive meta-analyses date from around 10 years ago. Since then, many more studies have been published, including on self-guided Internet-based TD-CBT, a highly scalable format with great potential to reach many people. Our new systematic review clarifies whether TD-CBT works just as well in different settings, is equally as effective as DS-CBT, and if its effects hold up over the long term, i.e., years, not just months.
To base results on the best evidence, we investigated only RCTs. Studies tested adult patients with emotional disorders who underwent TD-CBT and were compared to a control group. For a comprehensive update, we included various controls besides DS-CBT such as wait-list control, treatment-as-usual, or other active interventions. Our scope included various treatment formats: face-to-face (individual or group) and Internet-based (clinician-guided or self-guided). We evaluated effects on self-reported symptoms of anxiety and depression at post-treatment and later follow-up assessments.
We preregistered our plan, conducted the study, wrote up the manuscript and submitted it to a scientific journal. Although it was reviewed, our paper was ultimately rejected – a common fate. We received helpful feedback, but momentum was lost and amidst staff changes and the emerging COVID-19 pandemic, the paper was eventually filed away. It was only picked up again in 2022 when a new postdoc (me!) thought they would like to learn to conduct a meta-analysis and that it would be a quick job to update the review. We had planned to simply resubmit a slightly more polished version of the existing draft. Alas, we soon realised that many more studies had been published since our search and the project would involve a lot of work. Nevertheless, we decided to embrace the challenge and opted to redo the entire analysis using open-source software so that we could make our code available along with the manuscript.
Two independent reviewers from our team screened search results from multiple databases for new studies that met our inclusion criteria. They extracted the necessary data to conduct the meta-analysis and evaluated the quality of the included studies, checking for any biases in the way these were designed, conducted, analysed, and reported. We used methods such as random-effects models which consider heterogeneity between studies to provide a more robust result.
Once again, we finalised our manuscript and submitted it to another journal. This time, however, we did not even receive feedback; our paper was rejected outright, citing a lack of relevance to the outlet. But about the same time I added this new sticker to my rejection collection, we also received a curious email. A senior editor at Nature Human Behaviour had read our preprint and invited us to publish the paper with them. This did not seem real! It was only after double-checking with the editorial team that we ruled out a scam and began to feel excited. Our beliefs in open science and in our study intact, we set out to update our search yet again to comply with the journal’s rigorous policy of reporting up-to-date evidence. In addition, we conducted several sensitivity analyses to corroborate our findings, thanks in part to helpful comments from constructive reviewers.
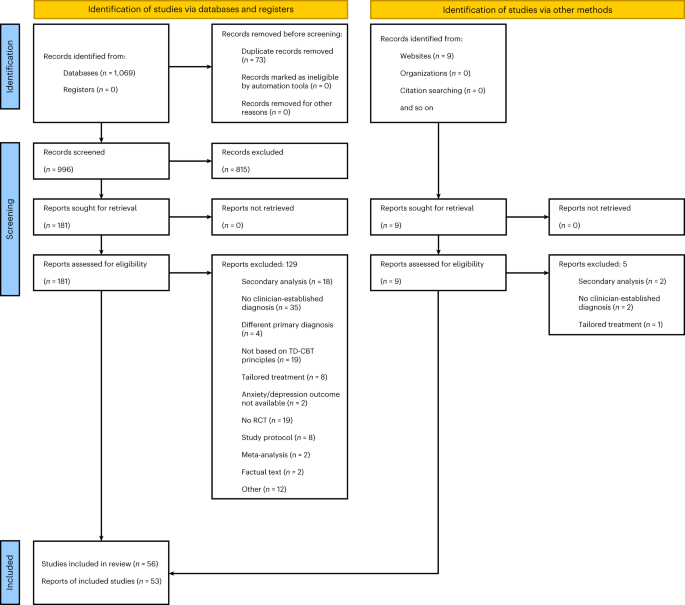
We found 56 eligible RCTs, half published after 2019, which comprised 6,916 patients in total. The majority tested the effectiveness of TD-CBT in a group setting compared to a wait-list condition. Eight studies included a DS-CBT comparison group and around 75% re-assessed patients at least once following completion of treatment (typically after three or six months).
For our meta-analysis, we examined a subset of 53 RCTs including 6,705 patients in total. This investigation revealed that overall, TD-CBT reduced symptoms of anxiety and depression significantly more than control conditions. It did not matter much in which setting the therapies were conducted, individual, group, and Internet-based formats were similarly beneficial. A direct contrast with DS-CBT showed that TD-CBT was just as effective with no statistically significant difference. Comparisons with wait-list and treatment-as-usual, however, confirmed TD-CBT as clearly superior with large effects. It also showed stronger symptom reduction in contrast to other active therapies, though only for depressive symptoms. Patients who had received TD-CBT reported better mental health compared to control patients for up to one year after treatment. It is especially encouraging that studies which made use of Internet-based formats to provide the therapy showed large and stable long-term effects as well.
While the assessed studies differed somewhat in design and were of mixed quality, they comprise a rich data set including several thousand patients. Moreover, though lengthy and sometimes frustrating, the process of continuously updating and improving our search and analyses resulted in a thoroughly researched and transparently reported study which we are proud to present. Our meta-analysis provides a substantial contribution to the field and strengthens the evidence base for transdiagnostic psychotherapy. TD-CBT can help close the treatment gap and better meet an increasing demand for psychotherapeutic intervention. We hope that our study gives further encouragement to therapists and healthcare professionals to employ TD-CBT.
Follow the Topic
-
Nature Human Behaviour
Drawing from a broad spectrum of social, biological, health, and physical science disciplines, this journal publishes research of outstanding significance into any aspect of individual or collective human behaviour.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Digital Media and Mental Health
Publishing Model: Hybrid
Deadline: Oct 30, 2026
Basic Psychological Needs and Well-Being
Publishing Model: Hybrid
Deadline: Nov 27, 2026

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in