Considering Patients' Perspectives and Expectations for OnabotulinumtoxinA Treatment and Physiotherapy and Rehabilitation Treatments in Chronic Migraine Patients
Published in Healthcare & Nursing, General & Internal Medicine, and Pharmacy & Pharmacology

OnabotulinumtoxinA and Chronic Migraine
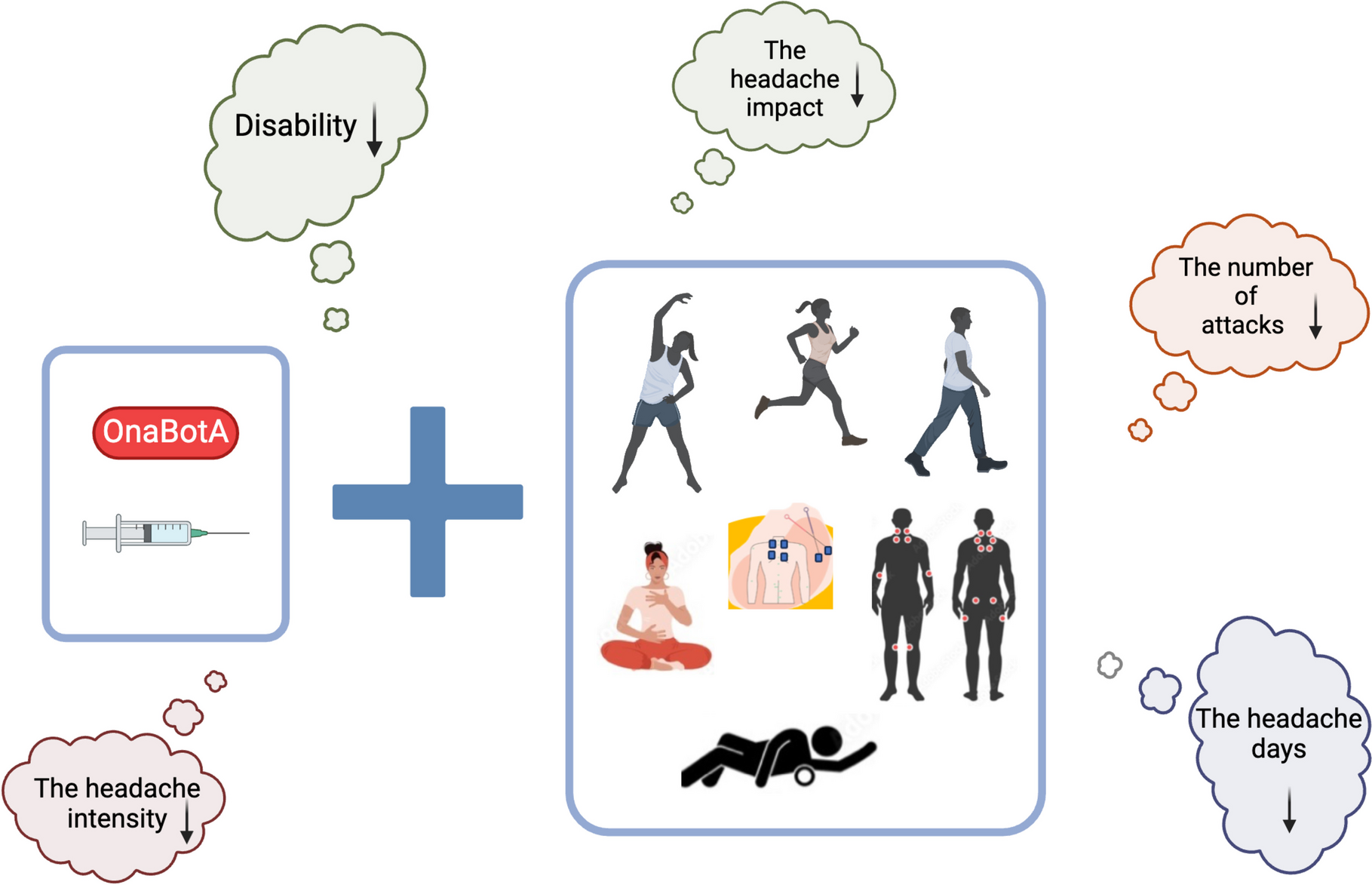
OnabotulinumtoxinA (OnaBotA) is administered to targeted head and neck muscle areas every three months to treat chronic migraine. It offers benefits such as reducing the number of headache days, frequency of attacks, headache intensity, disability, and improving quality of life (QoL). In addition to its limited effect duration of 3–4 months and the fact that OnaBotA treatment may not be covered by health insurance in hospitals, holistic complementary approaches are also recommended to prevent possible side effects from OnaBotA, reduce patients' dependence on medical treatments, support treatment compliance, and actively involve patients in migraine management.
So What Are Physiotherapy and Rehabilitation Treatments, Which Are Holistic Complementary Approaches?
Physiotherapy and rehabilitation treatments (PRT), exercises, hot-cold applications, electrical stimulation, massages and mobilizations, manipulations, and manual treatments such as osteopathy, which are the basic components of holistic complementary approaches, have minimal side effects and actively involve patients in the treatment processes.
Possible Benefits of OnabotulinumtoxinA and Physiotherapy and Rehabilitation Treatments When Applied Together
Considering the areas where OnaBotA is applied, strengthening the muscles in the head and neck, stretching the tissues to reduce stiffness, and improving cervical posture may increase the effectiveness of the treatment. Exercises, manual therapy and soft tissue release methods can provide varying degrees of PRT in the treatment of CM. In addition to OnaBotA application, which requires a repeat after 3–4 months, providing PRT applications that can show benefits over 3–4 months may lead to long-term improvements.
These treatments are reported to be applied less frequently in clinical migraine care, which may lead to healthcare professionals rarely prescribing PRT to patients. In some cases, patients may not have access to a physiotherapy and rehabilitation clinic dedicated to migraine in their hospital or city, potentially limiting their awareness of PRT options. Therefore, it is also important to consider patients' opinions regarding these treatments. In this study, we aimed to explore CM patients' perspectives and expectations regarding PRT combined with OnaBotA. Understanding these perspectives will help plan and implement evidence-based physiotherapy and rehabilitation strategies.
What did we find?
- PRT was recommended for 41.8% of the patients who received OnaBotA, compared to 18.9% in the group that did not receive OnaBotA. Neurologists were the primary recommenders for the OnaBotA group (38.2% vs. 7.5% in the group that did not receive OnaBotA).
- The percentage of patients who received neck stabilization exercises (12.7%) and pilates (12.7%) was higher in the OnaBotA group.
- The percentage of patients who received all expectations regarding PRT was higher in the OnaBotA group (76.4%) than in the group that did not receive OnaBotA (33.8%).
- The improvements in migraine symptoms in patients who received OnaBotA and PRT together were in disability, headache intensity, headache impact, number of attacks, and headache days.
- The responses to the question “How many months of physiotherapy and rehabilitation treatment do you think you need to get better?” were 3.83 ± 1.17 in the OnaBotA group and 3.06 ± 2.64 in the group non-receiving OnaBotA.
- The percentage of those who wanted to receive treatment from physiotherapists specializing in migraine was 96% in the OnaBotA group and 94% in the non-receiving group.
- The percentage of those who had easy access to physiotherapy and rehabilitation treatment was 34% in the OnaBotA group and 30% in the non-receiving group.
- Our findings provide insights into the potential benefits of combining OnaBotA with physiotherapy and rehabilitation in managing CM. Patients receiving OnaBotA may benefit from complementary therapies and may improve their overall treatment experience. Patients appear motivated to increase their awareness and participation in the treatment process.
Notes for Future Studies
- Future research should focus on conducting randomized controlled trials to systematically evaluate the combined effects of OnaBotA and PRT.
- Such studies should include larger sample sizes, standardized intervention protocols, and objective measurements to assess the benefits and limitations of this combined therapeutic approach.
- They should aim to provide robust evidence to guide clinical practice and improve patient outcomes in migraine management.
Follow the Topic
-
SN Comprehensive Clinical Medicine
A broadly based, peer reviewed journal that publishes original research in all disciplines of clinical medicine and their subspecialties, including all aspects of Imaging, Surgical and Medical studies related to diagnosis, treatment and management.

Related Collections
With Collections, you can get published faster and increase your visibility.
Environmental and Lifestyle risk factors for Non-Communicable Diseases
Research pointing at the role of environmental and lifestyle risk factors towards increased burden of Non-Communicable Diseases (NCDs) is fragmented in consideration of the large span of risk factors. Some of them are largely studied, e.g. air pollution, tobacco smoking, alcohol use, whereas other are less extensively studied: for example, exposure to noise, or some dietary risks (e.g. low consumption of nuts and seeds, low intake of omega-3 fatty acids). Moreover, many analyses focus on one-to-one associations between risk factors and NCDs. The overall effect of this is that a global picture of the effects of environmental and lifestyle risk factors is difficult to gather, with very few exceptions (e.g. smoking or high blood pressure). In addition to this, the “targets” of risk factors are not evenly addressed, and include risk factors for disease onset, risk factors for mortality and risk factors for disease progression (each with its own definition of progression).
This collection is aimed to provide an overview on the main risk factors for NCDs. Submissions are mostly welcome in the format of literature reviews, either systematic or narrative, that provide an appreciation of the impact that risk factors have on mortality and morbidity of selected NCDs. Contribution might be either disease-oriented (e.g. exploring the risk factors for stroke), or risk oriented (e.g. exploring which diseases are associated to low physical activity).
The specific requirements are:
1) to compare the results gathered in the contribution against the most recent estimates that can be produced by the Global Burden of Disease (GBD) study, thus showing what the manuscript adds to the state of knowledge in a GBD perspective;
2) to specifically link the results to the UN Sustainable Development Goals (SDGs), thus showing the potential impact of implementing policies towards risk reduction or elimination in light of global health improvement.
Publishing Model: Hybrid
Deadline: Mar 31, 2027
Talent Honors Program 2026
This article collection will welcome research or review articles authored by Early Career Researchers (PhD/PostDoc or Resident) on any topic covered by the journal.
Applications can be made by the submission of a Research or Review article (as the corresponding or co-corresponding author), within the scope of SN Comprehensive Clinical Medicine, to the article collection "Talent Honors Program 2026". Applicants should include a declaration of their eligibility in the cover letter alongside their submitted article.
15 articles will be published under this program and, if not published under an OA license (please check SN OA agreements for eligibility), they will be granted Free Temporary Access (FTA) for 4 months. FTA will be granted to 15 applicants on a first-come, first-served basis, upon acceptance and publication of their submitted article after peer review.
All submitted articles will be sent for an initial round of peer-review, regardless of novelty, provided they are in scope and sufficiently sound. Articles will follow the journal's standard peer-review process, with the collection edited and overseen by the Editor-in-Chief.
The program will close to submissions October 31st, 2026, or once the total number of published articles has been reached.
Successful applicants will also be considered for the role of guest editor for a new collection planned for 2027. To apply, they will need to submit a proposal for a prospective article collection, in which they would serve as junior guest editor under the guidance of a senior member of the editorial board. All proposals will be reviewed by the Editor-in-Chief, and only one or two projects will be selected for implementation each year.
Additionally, successful applicants will be invited to join the Editorial Board of the journal as Junior members.
Publishing Model: Hybrid
Deadline: Oct 31, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in