Developing a Clinically Translational AI Model to Predict Immunotherapy Response
Published in Cancer, Computational Sciences, and Biomedical Research
Cancer immunotherapy has transformed cancer treatment over the past two decades. Despite its success, only about 20-30% of patients respond to immunotherapy, with variations across different cancer types. This variability underscores the urgent need for biomarkers that can predict patient responses more accurately. Currently, Tumor Mutational Burden (TMB) and PD-L1 expression are the primary biomarkers used, but their predictive power is limited.
Recent advances in measurement techniques and artificial intelligence have led to the proposal of numerous biomarkers. However, translating these biomarkers into clinical practice poses significant challenges. Many proposed models are "black box" models that lack interpretability. They often fail to generalize well across different patient cohorts. Some models rely on sophisticated, time-consuming, and costly measurements that are not yet routine in clinical settings.
Our motivation was to develop a model that could be used clinically. To be viable, the model must surpass current biomarkers like TMB and PD-L1 in performance, be robust across various datasets, use routinely measured clinical data, and be interpretable to clinicians.
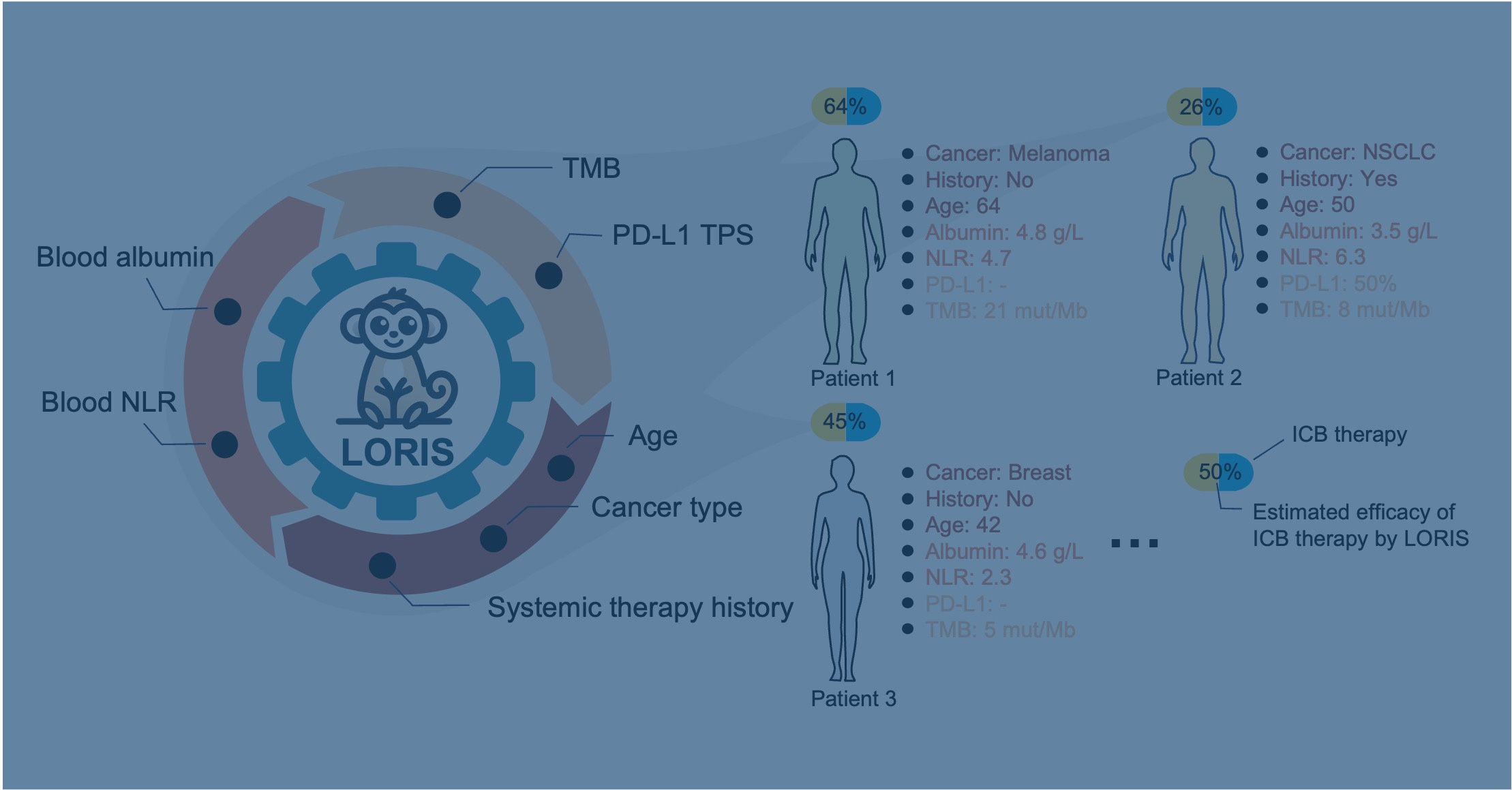
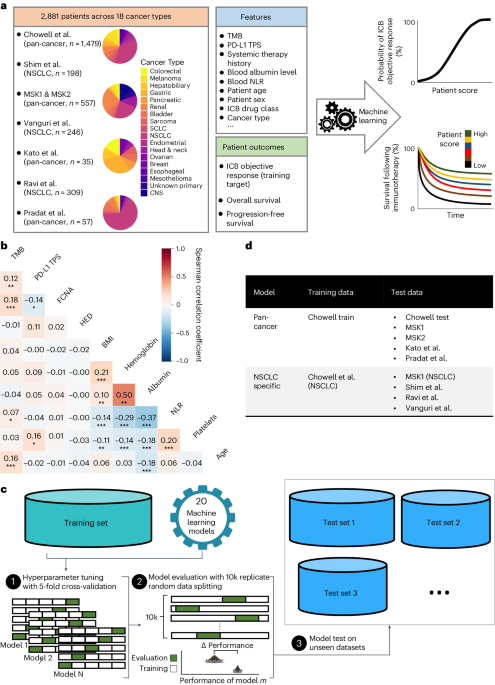
With these criteria in mind, we developed LORIS, a transparent and interpretable model. LORIS uses six routinely measured patient features: tumor mutational burden, age, cancer type, therapy history, and two blood metrics—albumin and neutrophil-to-lymphocyte ratio. We compared LORIS to 20 other machine learning models that use more features or have more complex structures. Remarkably, LORIS outperformed all of them in cross-validation. Moreover, it exhibited the smallest performance difference between training and cross-validation, as well as on external validation datasets, indicating a minimal risk of overfitting. It is worth mentioning here that the issue of overfitting has not been adequately addressed in many previous studies, even those published in top journals.
Another standout feature of LORIS is its ability to predict immunotherapy response probabilities in a clear, monotonic manner. For instance, a LORIS score of 0 corresponds to a near 0% response probability, while a score of 1 indicates a near 100% response probability. This is in contrast to TMB, where even low TMB patients can still have a 20% response probability.
The clinical implications of our work are significant. LORIS can identify patients who were previously considered poor candidates for checkpoint inhibitors, such as those with low TMB or PD-L1 expression. We hope this finding will enable more effective use of immunotherapy in these specifically selected patient populations, thus advancing precision medicine.
Follow the Topic
-
Nature Cancer
This journal aims to provide a unique forum through which the cancer community will learn about the latest, most significant cancer-related advances across the life, physical, applied and social sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Cancer Neuroscience: from mechanisms to therapy
Publishing Model: Hybrid
Deadline: Jan 30, 2027


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in