Emerging issue in cancer genetics: counseling carriers of reduced penetrance pathogenic variants
Published in Healthcare & Nursing, Cancer, and Genetics & Genomics
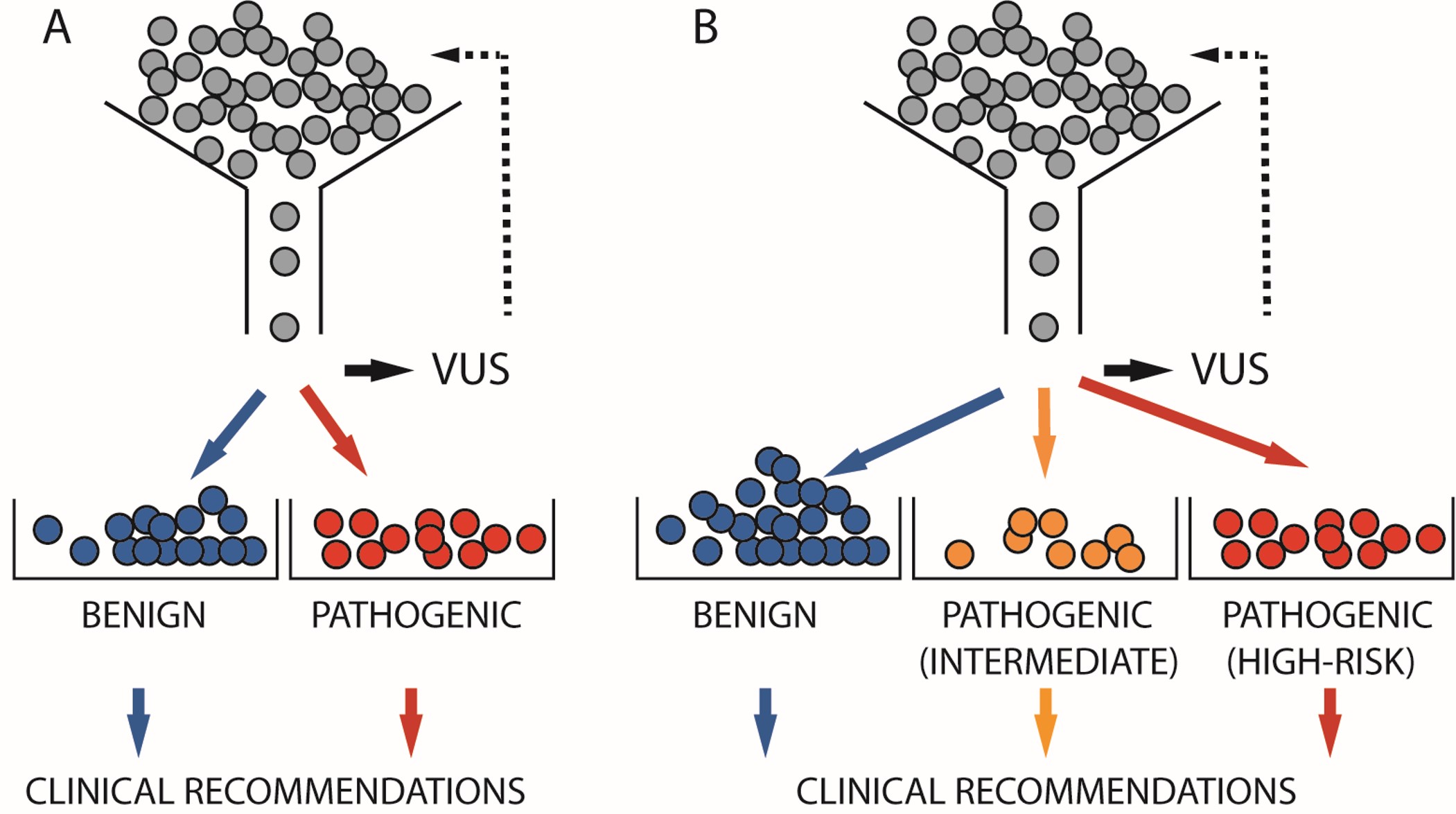
Since genetic testing for BRCA1 and BRCA2 became available nearly 30 years ago, identified variants have been classified as either clinically actionable or not. Non-actionable variants, which include benign, likely benign, and variants of uncertain significance (VUS) according to the American Board of Medical Genetics and Genomics (ABMGG) classifications, generally pose an unknown risk or a risk similar to that of the general population and should not influence enhanced medical management. Clinically actionable variants, encompassing likely pathogenic and pathogenic categories as per ABMGG, typically confer a risk that is 4 to 10 times higher than that of the general population. Over time, clinical management guidelines for affected and unaffected carriers were developed based on this non-actionable/actionable dichotomy.
Molecularly, most benign variants were silent (a nucleotide change without changing the amino acid residue) or non-coding changes with no effect on the protein or its splicing. Pathogenic variants were represented primarily by frameshift or nonsense changes resulting in complete loss of function. Because the impact on the transcript or the protein for these types of variants could be inferred from sequence alone, they also fit well in the benign/pathogenic dichotomy. However, most missense changes (replacing one amino acid residue for another) ended up in a catch-all category of variants of uncertain clinical significance because the impact on protein is more difficult to predict.
With the development of functional assays for BRCA1 and BRCA2 variants, it became clear that many missense and splicing variants had a significant adverse impact on function but may or may not lead to a complete loss of function. In fact, large scale assays showed a spectrum of activity, raising the question of whether they would confer a similar spectrum of risks (if risk was a continuum) or if there would be a specific threshold below which all variants would confer similar, highly elevated risk (if risk was discrete).
In parallel, observations from clinical testing companies and clinical geneticists, suggested the existence of families that seemed to have elevated risk, but a familial pattern that was not as severe as families with complete loss-of-function pathogenic variants. Over the years, these variants were often classified in the catch-all bucket of VUS or in non-standardized new categories including ‘lower’ or ‘reduced penetrance’, ‘atypical risk’, pathogenic ‘light’ and ‘special interpretation, see below’. Combined with the results from functional assays, these observations supported the idea that risk exists on a continuum. Three immediate problems became evident. First, when these variants were classified as VUS yet were pathogenic, at the penetrance level they still conferred risk albeit lower compared to loss-of-function pathogenic variants, leading to potential for undertreatment. Second and conversely, some of these variants might have been classified as pathogenic thereby incorrectly implying they conferred a risk comparable to loss-of-function variants, which could lead to overtreatment, such as offering prophylactic surgery when not justified by their true risk profile. Third, even though risk is a continuum, clinical decisions are typically binary (Yes/No).
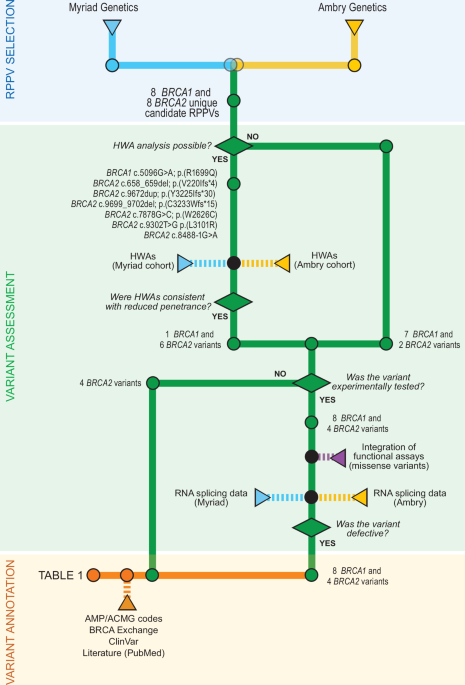
Our group decided that a way to overcome this impasse was to begin by identifying variants for which a minimal consensus could be reached, indicating that they represented variants of reduced penetrance (NPJ Precis Oncol. 2024 Nov 2;8(1):247). These variants could then be used as risk and functional yardsticks to create a new category of intermediate risk, for which specific risk-appropriate guidelines could be developed. This effort, which included two of the largest hereditary cancer testing companies in the US, identified 16 variants in BRCA1 and BRCA2 that had direct and indirect evidence to support atypical risk (RR 2-4). These variants showed a significant impact on function yet an attenuated personal and/or family history. Given the rarity of some of these alleles, risk-determining epidemiology studies may never be feasible. Functional assays may provide that bridge, when well calibrated, to identify rare variants in this new class of reduced penetrance pathogenic variants and allow for the proper counseling of carriers.
Next steps include some large-scale studies to determine the functional impact of the variants and estimate the risk of at least those with a high enough population frequency to better define their risks. Additionally, development of a framework to adjust both the interpretation and clinical recommendations according to the risk level of the carriers is essential. For the latter point, incorporation of other genetic (e.g. polygenic risk score) or non-genetic risk factors (e.g., hormonal, lifestyle) will be critical. Due to their very nature, risk estimates are unlikely to ever be precise, but the field should establish a well-founded, actionable risk threshold that the carrier and providers can use to make an informed choice.
Contributed by Tuya Pal, Erin Mundt, Marcy E. Richardson, Elizabeth Chao, Tina Pesaran, Thomas P. Slavin, Fergus J. Couch and Alvaro N.A. Monteiro
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Next-Generation AI in Drug Design for Precision Oncology
Publishing Model: Open Access
Deadline: Apr 01, 2027


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in