Rugengamanzi E 1,2, Manirakiza AVC 3,4, Fadelu T 5,6, Rebbeck TR 6,7
At the 2018 World Economic Forum Annual Meeting in Davos-Klosters, Switzerland, a session titled "Governing Advanced Technologies: Precision Medicine" sparked a transformative journey for Rwanda’s healthcare system. By 2019, the Rwandan government committed to integrating precision medicine into its healthcare framework to improve outcomes across multiple domains. This commitment led to a successful application for an NCI grant (R01 CA207365/CA/NCI) in collaboration with the Dana-Farber Cancer Institute (DFCI). Together, they initiated a landmark study investigating the genetics of breast and prostate cancers in the Rwandan population.
The challenges were significant. At the time, Rwanda lacked infrastructure for cancer genetic risk assessment, including counseling and testing services, and prior studies had been limited in sample size(1,2). The study began by establishing patient eligibility criteria based on the National Comprehensive Cancer Network (NCCN) guidelines for genetic testing specific to these two cancers(3,4). To ensure awareness and participation, a meeting was convened with clinicians from Rwanda's three main oncology referral centers—King Faisal Hospital, Rwanda Military Referral and Teaching Hospital, The University Teaching Hospital of Kigali (CHUK), University Teaching Hospital of Butare (CHUB) and the Butaro Cancer Center of Excellence. Study staff were trained in pre-genetic counseling, pedigree building, and the basics of cancer genetics to support this initiative.
Recruitment and Genetic Testing
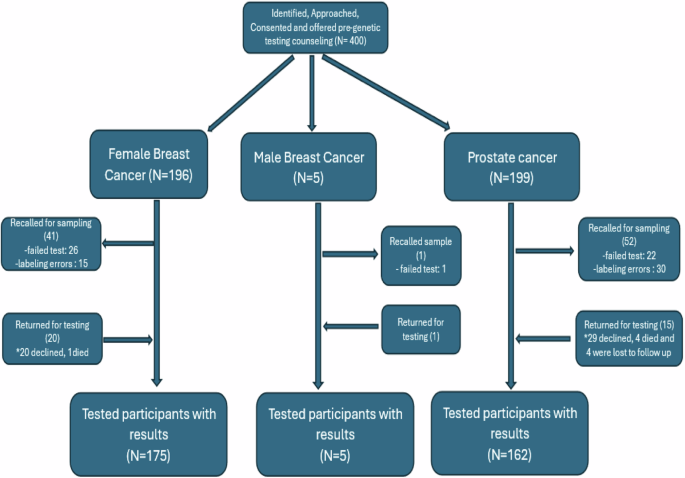
Recruitment commenced on April 2, 2022, starting with nine young women with breast cancer who consented to participate. Saliva samples were collected for logistical reasons, and subsequent testing was conducted using an 84-gene panel at Invitae Laboratories (San Francisco, CA). Over the next 10 months, 400 patients (201 with breast cancer and 199 with prostate cancer) were enrolled, making this the largest cancer genetics study in Rwanda and addressing a significant gap in Sub-Saharan African (SSA) cancer research, where genetic data remain scarce.
Findings and Implications
The study aimed to identify germline variations in key cancer-related genes in Rwandan breast and prostate cancer patients. Among 342 participants whose results were analyzed (180 with breast cancer—175 women and 5 men—and 162 with prostate cancer), pathogenic variants (PVs) were identified in 18.3% of female breast cancer cases, 20% of male breast cancer cases, and 4.3% of prostate cancer cases. BRCA2 emerged as the most frequently identified PV. Additionally, among non-PV carriers, 65% had one or more variants of uncertain significance (VUS). These results underscore the importance of integrating germline genetic testing into cancer care in SSA and demonstrate the feasibility of applying global guidelines like the NCCN criteria, even in resource-limited settings where comprehensive family histories are often unavailable.
Key Challenges and Solutions
- Risk Communication: Effective risk communication is essential to the success of cascade testing in SSA. Community participatory models can build culturally sensitive communication strategies, ensuring families understand genetic risks. Addressing language barriers, health literacy, and stigma through targeted education and counseling is critical. Leveraging technology and engaging communities can further enhance participation and trust.
- Establishing Familial Cancer Clinics: Creating one-stop familial cancer clinics that integrate genetic testing, counseling, and risk management would streamline care delivery. These clinics could maintain structured familial cancer registries, improve follow-up for cascade testing, and facilitate personalized interventions. Additionally, they could serve as hubs for data collection and research, advancing cancer prevention and treatment.
- Infrastructure Development: Incorporating genetic testing into routine cancer care requires investments in diagnostic laboratories, data management systems, and healthcare professional training in cancer genetics. Partnerships between local and international institutions can help bridge resource gaps, provide access to genomic technologies, and foster knowledge exchange. Strengthening this infrastructure will enable equitable integration of genetic insights into cancer care, reducing disparities across the region.
Future Directions
Building on this foundation, our next steps include:
- Understanding Patient Experiences: Conducting qualitative surveys to explore patient experiences of receiving genetic results (data analysis is currently underway).
- Cascade Testing: Developing strategies for disclosing results to at-risk family members and scaling up genetic counseling services.
- Capacity Building: Establishing familial cancer registries, enhancing laboratory infrastructure, and diversifying treatment options.
This research addresses critical gaps in understanding breast and prostate cancer susceptibility in Rwanda. By adapting global guidelines to local contexts and investing in genetic testing and counseling, Rwanda is emerging as a leader in precision medicine for resource-limited settings. Future studies will refine these approaches to ensure equitable and effective cancer care for all.
Reference
- Uyisenga JP, Segers K, Lumaka AZ, Mugenzi P, Fasquelle C, Boujemila B, et al. Screening of germline mutations in young Rwandan patients with breast cancers. Mol Genet Genomic Med. 2020 Sep 22;8(11):e1500.
- Habyarimana T, Attaleb M, Mugenzi P, Mazarati JB, Bakri Y, El Mzibri M. CHEK2 Germ Line Mutations are Lacking among Familial and Sporadic Breast Cancer Patients in Rwanda. Asian Pac J Cancer Prev. 2018 Feb 1;19(2):375–9.
- Daly MB, Pilarski R, Yurgelun MB, Berry MP, Buys SS, Dickson P, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 1.2020. J Natl Compr Cancer Netw JNCCN. 2020 Apr;18(4):380–91.
- Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology - PubMed [Internet]. [cited 2025 Feb 3]. Available from: https://pubmed.ncbi.nlm.nih.gov/31085757/
Affiliations
1: Oncology department, Butaro cancer center of Excellence, Butaro, Rwanda
2: Internal medicine, Clinical Division, University of Global Health Equity, Butaro, Rwanda
3: Oncology Unit, Department of Medicine, King Faisal Hospital, Kigali, Rwanda
4: College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda
5: Harvard Medical School, Boston, MA USA
6: Dana Farber Cancer Institute, Boston, MA USA
7: Harvard T.H. Chan School of Public Health, Boston, MA USA
Follow the Topic
-
npj Genomic Medicine
This is an international, peer-reviewed journal dedicated to publishing the most important scientific advances in all aspects of genomics and its application in the practice of medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Artificial Intelligence in Genomic Medicine
Publishing Model: Open Access
Deadline: Jun 23, 2026
The microbiome in precision medicine
Publishing Model: Open Access
Deadline: Sep 28, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in