How can we reduce the carbon footprint of cataract surgery pathways?
Published in Social Sciences, Sustainability, and General & Internal Medicine
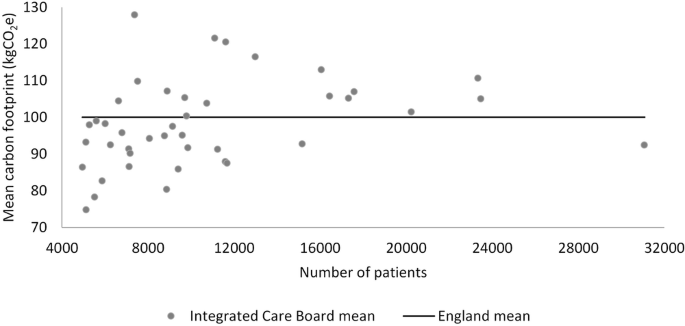
Using Hospital Episodes Statistics (HES) for 455,346 cataract procedures conducted in England during the financial year 2021/22 we identified the average carbon footprint of key elements of the cataract surgery pathways (from pre-operative assessment to post-operative follow-up) to be 100.0 kgCO2e. Had all Integrated Care Boards in England adhered to the GIRFT HVLC pathway for cataract surgery, then 17.5 kilotonsCO2e would have been saved in the year. Given the large volume of cataract surgery conducted in England each year, the savings potential is significant; key factors that may be amenable to change are pre- and post-operative contacts (many of which could be avoided through one-stop-shop models), patient-initiated follow-up (PIFU) and greater use of virtual appointments.
The idealised patient pathway had a carbon footprint of 61.5 kgCO2e. The pathway was developed with a focus on optimal patient care and service efficiency. There was no specific focus on environmental sustainability or carbon reduction. Our paper highlights the potential synergy between better care for patients, efficient and productive care delivery and environmentally sustainable practice. Where these three elements meet has been termed the ‘triple bottom line’.2
The Getting It Right First Time (GIRFT) programme within NHS England has a remit to reduce unwarranted variation in care provision that negatively impacts patient outcomes. Within this remit, GIRFT has developed standardised care pathways with a focus on efficiency and patient outcomes. However, with healthcare recognised as a major contributor to global carbon emissions (responsible for 4.6% of all carbon emissions in the UK) GIRFT is now adding a carbon reduction lens to its work and has started to investigate ways in which it can support the transition to net zero within the NHS in England.
Much of this work will involve reviewing current recommendations to better understand how they also help reduce the carbon emissions of the NHS, as we have done in this paper. However, the work will also consider aspects of care where improving environmental sustainability is the primary focus. While savings of carbon associated with reduced bed days and outpatient attendances can be counted at a patient- and procedure-specific level, they may be hard to realise and less tangible in practice, due to demand for services outstripping supply and the capacity released being taken up by other activity. Actions directly targeted at environmental sustainability (e.g. reduced use of single-use items in favour of reusable items, switching off theatre equipment when not in use and safe to do so) are likely to result in tangible savings. A balance of actions is needed.
GIRFT will shortly publish a guide to decarbonising the bladder tumour pathway in urological care. Recommendations include increased use of day case pathways, one-stop pre-assessment, minimising unnecessary imaging and enhanced recovery after cystectomy. This focus on sustainability is being extending to a number of other patient pathways in urology, and we are also expanding to look at elective orthopaedic surgery. Over time we hope to develop similar decarbonisation guides covering many of the 42 clinical specialties covered by the GIRFT programme.
The GIRFT programme has reach into every NHS hospital trust, Integrated Care Board (ICB) and region in England, and it is recognised that the programme can have a significant impact in the ambition for more environmentally sustainable healthcare in the clinical setting. In March 2024, research by a group of GIRFT clinicians published in Anaesthesia, the journal of the Association of Anaesthetists, concluded that GIRFT’s drive to reduce unwarranted variation in care and improve efficiency across the NHS put the programme in a unique position to identify exemplary practice which can be scaled nationally, as well as areas for improvement in sustainable healthcare.3
The research team identified several areas of GIRFT’s focus where there is the potential to contribute to a reduction in NHS carbon emissions, notably our work on: elective surgical hubs, which are ideal for trialling low carbon models of care and implementing sustainable methods; increasing rates of day case surgery, and; delivering a patient-centred service, for example, minimising face-to-face outpatient appointments one-stop-shop care models and virtual appointments.
The study also found there is great scope for impactful decarbonisation within GIRFT’s anaesthesia and peri-operative medicine (APOM) workstream. Studies have attributed 42% of the carbon footprint of surgical care to anaesthetic gases, and the GIRFT national report for APOM (2021) highlighted a number of areas where the carbon footprint for the specialty might be reduced, including reducing and recycling waste and clinician education on waste management; use of low-flow inhalational anaesthesia wherever possible; use of total intravenous anaesthesia; increased use of regional anaesthesia techniques; and increased use of augmented volatile anaesthetic gas capture.4
In addition, reducing operating theatre downtime can help to increase throughput and reduce the per-patient carbon emissions associated with running an operating theatre, such as lighting, heating, extraction systems and staff travel. In the longer term, once waiting lists have been reduced, operating theatre facilities and services could be turned off earlier in the day.
Assessing what a minimal surgery and anaesthetic procedure kit should contain for each procedure to eliminate unnecessary equipment would also help to avoid disposal or re-sterilisation of unused items.
Such transitions and more will be needed if the goal of net zero by 2045 is to be met.5
References
1. van-Hove M, Begum H, Phull M, et al. The carbon footprint of cataract surgery pathways in England: an observational study using administrative data. Eye (Lond) 2024.
2. Centre for Sustainable Healthcare. Sustainability in Quality Improvement (SusQI). 2024. https://sustainablehealthcare.org.uk/susqi (accessed 20th september 2024).
3. van Hove M, John JB, Ojelade E, et al. Unwarranted variation and the goal of net zero for the NHS in England: exploring the link between efficiency working, patient outcomes and carbon footprint. Anaesthesia 2024; 79(3): 284-92.
4. Snowden C, Swart M. Anaesthesia and perioperative medicine: GIRFT Programme National Specialty Report. London, UK: Getting It Right First Time, NHS England and NHS Improvement, 2022.
5. Greener NHS. Delivering a net zero NHS. 2022. https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/#:~:text=For%20the%20emissions%20we%20control,reduction%20by%202036%20to%202039 (accessed 6th March 2024).
Follow the Topic
-
Eye
The official journal of The Royal College of Ophthalmologists. Eye seeks to advance the science and practice of ophthalmology with the latest clinical and scientific research for clinicians, optometrists, orthoptists, other health care professionals and researchers interested in the visual sciences.

What are SDG Topics?
An introduction to Sustainable Development Goals (SDGs) Topics and their role in highlighting sustainable development research.
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Dry Eye Disease
Publishing Model: Hybrid
Deadline: Nov 25, 2026
Sustainability in Ophthalmology
Publishing Model: Hybrid
Deadline: Ongoing



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in