Impact of HIV exposure without infection on hospital course and mortality among young children in sub‑Saharan Africa: a multi‑site cohort study
Published in Biomedical Research, General & Internal Medicine, and Paediatrics, Reproductive Medicine & Geriatrics


Story behind the research:
This was a secondary data analysis from the Childhood Acute Illness and Nutrition (CHAIN) cohort study. The CHAIN study was a multi-country study that aimed to build an evidence base for the care of acutely ill malnourished children. In this study, I had an opportunity to collect data and provide clinical care to the study participants. As we kept discussing different participants in our study calls, we realized that the trajectory of children born to HIV-positive mothers, even when they had no HIV infection, was seemingly different from that of children born to HIV negative mothers.
Fast-forward, when I was doing my master’s degree in Public Health, I needed a research topic for my master’s dissertation. I wanted to compare different clinical outcomes among HIV positive children vs. HEU children vs. HIV-unexposed children. On further discussion with my research supervisor, it became clear that the outcomes of HIV positive children were known, and the knowledge gap was among the HEU vs HUU children. After identifying the research topic, I engaged my mentor (senior author), who reviewed my concept and supported me in getting the data request approved by the CHAIN Network. I did the data analysis, wrote my dissertation, and it was approved.
After surmounting that hurdle, the next step was transforming all the work from dissertation to manuscript format. That took some time. The senior author did extensive reviews, which necessitated changing a few things. The next step was circulating the draft to the co-authors, who provided detailed comments. Some comments required significant changes in analysis strategies, others required a change in the flow of content. It took me about one and a half years to transform the dissertation document into the first draft manuscript submitted to a scientific journal!
Why is the research valuable?
Successful Prevention of Mother to Child Transmission(PMTCT) interventions have resulted in a significant decrease in children infected with HIV and a high number of children who are HIV-exposed but not infected (HEU). In 2022, there were an estimated 15.4 million HEU children, with close to 90% residing in sub-Saharan Africa. Several studies have demonstrated an increased risk of morbidity and mortality among HEU children compared to HIV unexposed, uninfected (HUU) children. However, the drivers of mortality and morbidity among the HEU children remain unclear, which impedes efforts to improve outcomes in this vulnerable group. There have been few studies examining risk factors for poor outcomes among HEU children. In this study, the examined associations between HIV-exposure and mortality, nutritional status, illness severity at admission, hospital length of stay, and utilization of hospital resources. This analysis provides insight into the drivers of poor outcomes among HEU children. This contributes to the evidence for formulating interventions and further research for this vulnerable group of children.
What did the authors do?
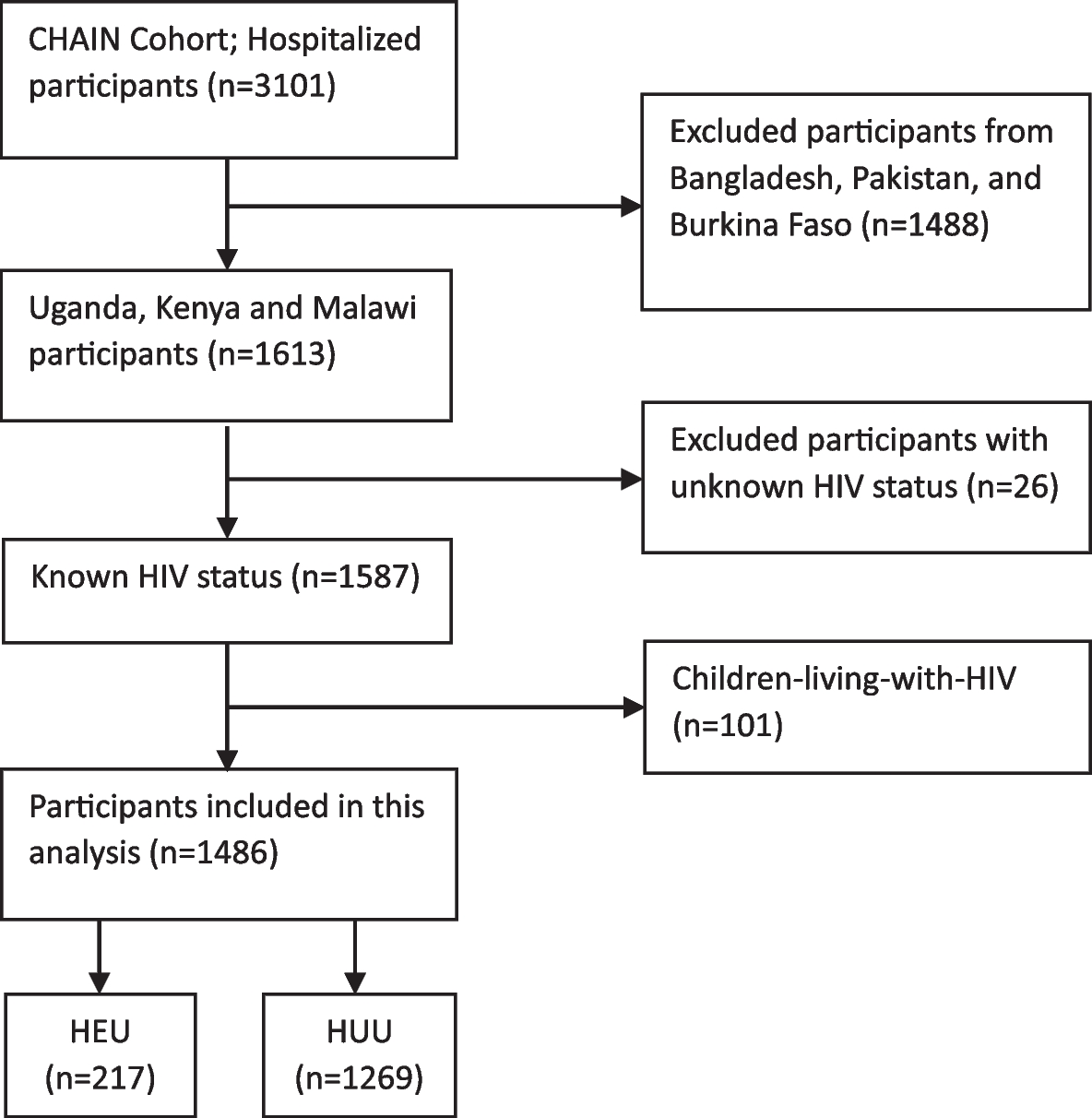
We did a secondary analysis of the CHAIN cohort study data. We analysed data from five CHAIN sites: Kampala (Uganda), Blantyre (Malawi), Migori (Kenya), Mbagathi (Nairobi, Kenya), and Kilifi (Kenya). A child was considered HEU if their mother was known to be living with HIV while pregnant, and the child’s confirmatory HIV test was negative, and/or a child < 18 months old had positive HIV rapid tests and the child’s confirmatory HIV DNA-PCR test was negative. We examined inpatient mortality and death within 30 days of admission among HEU children using logistic regression and survival analysis, respectively. We compared nutritional status (wasting and stunting), illness severity (high and low scores), and hospital length of stay (short or prolonged) using logistic regression. To assess the effect of HIV exposure on the occurrence of daily danger signs and resource utilization (oxygen use, nasogastric tube use, and antibiotic switch), days with any danger sign or the use of a specific resource were counted. A zero-inflated negative binomial regression model was applied because the days with a danger sign or use of any resource had leading zeros. In all the regression models, adjustment for appropriate child, caregiver, and household-level variables was done.
What did the researchers find?
HEU children had a higher risk of inpatient and 30-day mortality, were at an increased risk of wasting and stunting, and required a longer hospital stay, as compared to HUU children. There was no significant association between HIV exposure and illness severity, and no significant differences in the frequency and types of danger signs reported, as well as no differences in the requirement of hospital resources.
What are the implications of this study?
HEU children under 2 years of age are uniquely vulnerable to dying during hospitalization and the early post-discharge period, regardless of nutritional status. HEU children may be more vulnerable to undernutrition due to inadequate feeding practices, driven by a low prevalence of breastfeeding and a higher household food insecurity. The presence of sub-clinical infection(s) or acquisition of nosocomial infection(s) may have been more likely to complicate recovery among HEU children, resulting in prolonged hospital stay. Prolonged hospitalization not only places HEU children at increased risk for hospital-acquired infection and emergence of antimicrobial resistance but also increases the financial burden on the family, which further complicates the economic situation of these households.
Are there broader implications or applications of these findings? If so, what are they? What are the obvious limitations or caveats?
Our findings suggest that HEU children should be considered a high-risk population during hospitalization and in the early post-discharge period, regardless of perceived illness severity and nutritional status at admission
Additional biological factors that we were unable to quantify in our analysis, such as intestinal dysbiosis, metabolic derangements, and/ or subclinical infections such as cytomegalovirus, could have also contributed to wasting and the poor outcomes observed among HEU children.
What are the obvious next questions or steps to take this further? Are there aspects of the research that could be made stronger?
Longitudinal studies, preferably beginning in pregnancy, are likely to be required to understand how perinatal HIV exposure in the absence of infection compromises early childhood health. Identifying biological drivers of increased hospital mortality, wasting, and prolonged hospitalization among HEU children is essential to develop clinical care guidelines tailored to support this unique and vulnerable population.
Follow the Topic
-
BMC Medicine
This journal publishes outstanding and influential research in all areas of clinical practice, translational medicine, medical and health advances, public health, global health, policy, and general topics of interest to the biomedical and sociomedical professional communities.

Related Collections
With Collections, you can get published faster and increase your visibility.
Advancing research and management of menopause
BMC Medicine is calling for submissions to our new Collection, Advancing research and management of menopause, focusing on new perspectives and care practices that support individuals during this significant life transition. This Collection seeks to advance the understanding and management of menopause by gathering clinical research on its physiological, psychological, and social dimensions. We welcome submissions that explore topics such as perimenopause, menopausal symptoms, early menopause, and menopausal hormone therapy (MHT) but also innovative interventions that help individuals navigate menopause beyond pharmacological treatment.
The menopause journey, encompassing the climacterium and the natural conclusion of reproductive years, is a pivotal phase in the lifecycle that impacts health and well-being. This Collection aims to consolidate research that addresses the multifaceted aspects of menopause, including its physiological, psychological, and social dimensions, thereby offering a comprehensive view of the experiences faced during this transition.
Advancements in the understanding and management of menopause have opened new avenues for improving health. Research indicates that the heterogeneity of menopause (surgical, spontaneous, induced, early) as well as the heterogeneity of MHT (formulations, duration, age of initiation relative to menopause onset, cyclicity, progestrogen/progestin) can differentially affect outcomes, yet are not as well understood or studied. Studies on menopausal symptoms have enhanced our understanding of their prevalence and impact on daily life. Research on menopausal hormone therapy has evolved, shedding light on its benefits and risks, while growing evidence highlights a number of other effective options for managing common menopausal symptoms. Additionally, the focus on long-term effects of menopause, e.g. osteoporosis and prevention strategies, underscores the necessity for ongoing research and tailored interventions during and after this transition.
Continued exploration in this field promises to yield significant insights, potentially leading to the development of novel therapeutic options, personalized management strategies, and a broader understanding of the heterogeneity of menopause and individuals’ experiences. As research progresses, we may see improved guidelines for addressing early menopause and premature ovarian insufficiency, ultimately empowering individuals to navigate this life stage with confidence and health.
Topics of interest include but are not limited to:
- Management strategies for menopausal symptoms
- MHT: risks and benefits
- Post-menopausal osteoporosis prevention
- Ovarian aging and its implications
- Understanding early menopause and premature ovarian insufficiency
This collection supports and amplifies research related to SDG 3: Good Health & Well-Being and SDG 5: Gender Equality.
Publishing Model: Open Access
Deadline: Oct 17, 2026
Cardiac immunity and inflammation
BMC Medicine invites submissions to a new Collection focused on the interplay between cardiac immunity and inflammation. We welcome original research, translational studies, and comprehensive reviews that elucidate the underlying mechanisms, clinical consequences, and therapeutic opportunities arising from immune-cardiac interactions. By highlighting the importance of this link, we aim to foster collaboration and advance our understanding of how to improve patient outcomes in heart disease.
The intersection of immunity and cardiovascular biology represents a transformative frontier in modern medicine. Recent studies have highlighted the role of immune responses in various heart conditions, including myocarditis, cardiac xenotransplantation, and heart failure. Inflammation is increasingly recognized as a contributing factor to the pathogenesis and residual risk factor of cardiovascular diseases. This Collection aims to explore the mechanisms by which immune responses influence cardiac function, the role of clonal hematopoiesis and heart disease, and the implications of such interactions for cardiac outcomes.
Understanding cardiac immunity and inflammation is crucial for developing more targeted therapies and accurate CVD risk prediction. Past advances provided insights into the inflammatory processes involving cardiovascular conditions, leading to innovative approaches for diagnosis and treatment. For instance, the identification of biomarkers such as C-reactive protein enhances our ability to assess inflammation in patients with cardiovascular disease. Furthermore, the intersection of cardio-oncology has opened new avenues for research into how cancer therapies influence cardiac immune responses, emphasizing the need for a multidisciplinary approach to patient management.
Continued research in this field holds promise for unveiling drug discovery targets and strategies to mitigate inflammation-related cardiac damage. As we deepen our understanding of the immune mechanisms at play, we may see the development of more clinically relevant models of human disease and precision medicine approaches tailored to individual patients. The integration of this knowledge with advancements in technology, such as biomarker discovery and imaging techniques, could revolutionize the way we approach cardiac care.
Topics of interest include (but are not limited to):
- Role of immunity in cardiovascular biomedicine
- Systemic and cardiac-specific inflammatory pathways
- Residual inflammatory risk, e.g. “SMuRF-less but inflamed”
- Cross-organ communication and immune crosstalk
- Structural and functional cardiac remodeling driven by inflammation
- Novel biomarkers and prediction models
- Clonal hematopoiesis
- Cardio-oncology & therapy-induced immune modulation
- The role of immunity in cardiac xenotransplantation including partial heart transplantation
- Exposome/environmental exposures
- Epigenetic regulation of cardiac immunity and inflammation
- Immune memory and trained immunity in cardiovascular contexts
- Multi-omics integration (epigenomics, transcriptomics, proteomics) in cardiac disease
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3 (Good Health and Well Being).
Publishing Model: Open Access
Deadline: Feb 01, 2027



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in