Increased household transmission of Omicron variant compared to Delta, evidence from Norwegian contact tracing data
Published in Healthcare & Nursing

At the end of November 2021, the SARS-CoV-2 virus variant Omicron was detected in Norway. This was at a time when vaccination, as a strategy for controlling the pandemic in Norway, seemed to have a satisfactory effect. However, a Christmas party late November that year resulted in 74% of the participants being infected, even though 98% of them had two doses of vaccine. Omicron rapidly became the dominant circulating virus variant. The newly detected variant clearly had different properties than the existing Delta variant, and the need for knowledge about these properties was pressing.
The aim of our study was therefore to investigate the transmissibility of and susceptibility for the Omicron variant for different categories of vaccinated individuals, and compare these properties with the properties of the more investigated Delta variant.
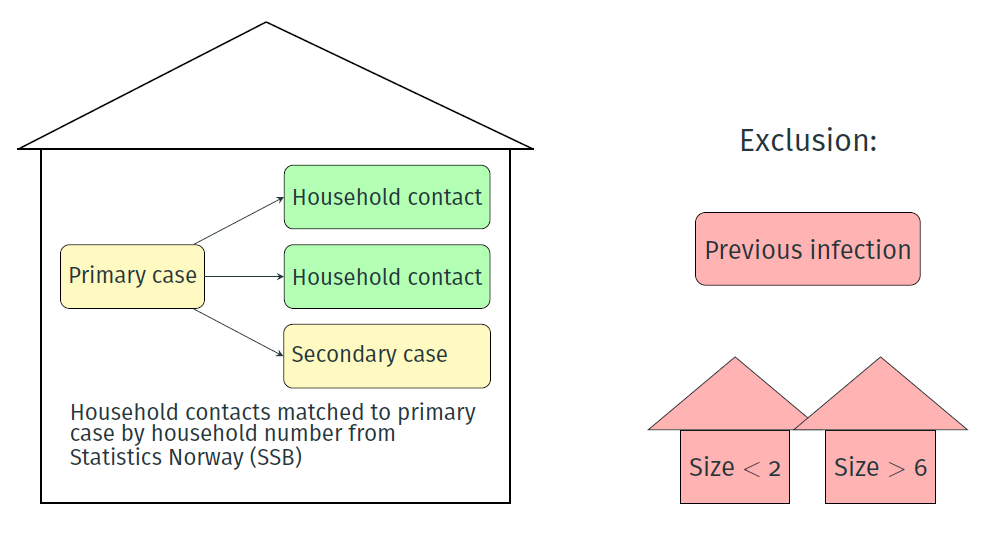
We had access to contact tracing data through the Norwegian Pandemic Preparedness Registry, Beredt C19 [1]. Contact tracing is in Norway carried out through phone interviews performed by trained health personnel. First, we identified primary cases in the data. A primary case was defined as a positive case who were not listed as anyone’s contact. This is then the person that initiated the contact tracing in the household. Traced contacts with matching household number to their primary case were then extracted, as illustrated in Figure 1. The study period was December 14, 2021 until January 23, 2022. We only included primary cases until January 13, 2022, to ensure a 10-day exposure of all contacts. The resulting data set consisted of 2169 household contacts (60% Omicron households and 40% Delta households).
The household secondary attack rate (SAR), vaccine efficacy (VE) and risk ratio (RR), stratified by covariates as age, vaccine status of contacts or primary cases and gender, were estimated through a binomial regression. Although other methods, like the chain binomial model, may give less biased estimates, we found the binomial regression model to be best suitable for the data we had available.
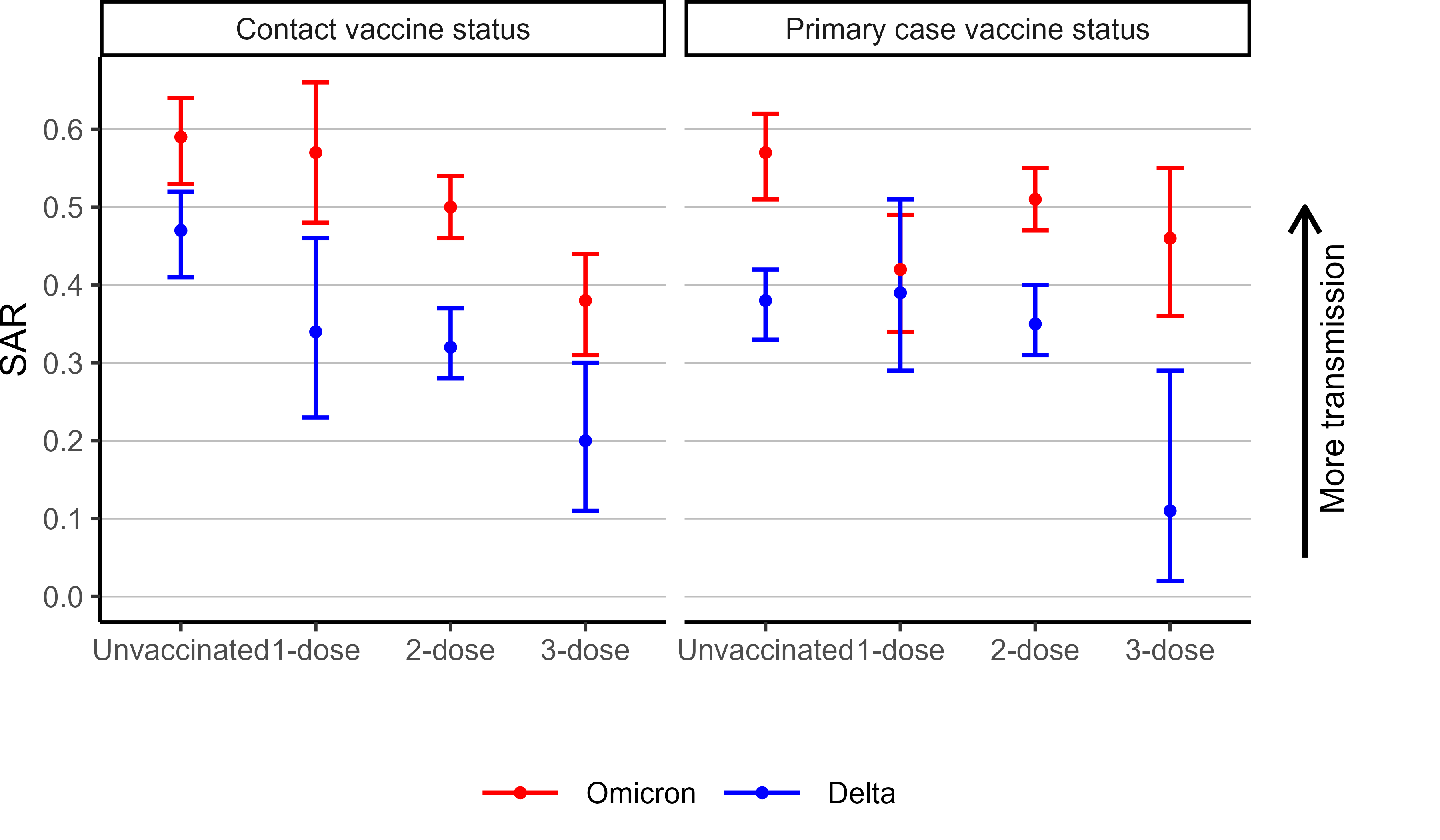
Not surprisingly, we found a higher overall 10-day household secondary attack rate (SAR) of Omicron compared to Delta. Furthermore, when conditioning on the vaccine status of either the primary cases or the contacts, the Omicron variant had a significantly higher risk of both transmission and infection compared to Delta, as seen in Figure 2.

Figure 2. Secondary attach rate stratified by vaccine status and variant for contacts and primary cases separately.
By stratifying the analysis by the vaccine status of the primary cases, the estimated vaccine effectiveness (VE), or equivalently the risk ration (RR), tells how effective the vaccine is for preventing transmission in the household. By stratifying by the vaccine status of the contacts, the estimated VE tells how effective the vaccine is for preventing infection or similarly, reducing the susceptibility of contacts. The protection by vaccination showed different properties for transmission and infection in Omicron households. The results in Figure 3 shows that the RR of transmission did not decrease with increased number of vaccine doses in the primary cases (red lines). The Delta variant however, show a clear decrease in RR (blue lines).

Figure 3. Risk ratio (RR) of transmission, for the different vaccination groups compared to the unvaccinated group, for Omicron and Delta variants separately.
Another story can be read if we instead stratify by the vaccine status of the contacts, as shown in Figure 4. The VE for both Omicron and Delta increases as the number of vaccine doses increases, even though the VE are in general lower for Omicron than Delta.

Figure 4 Vaccine effectiveness (VE) against infection, for the different vaccination groups compared to the unvaccinated group, for Omicron and Delta variants separately
The aim of using contact tracing data, rather than doing a pure registry based study, is that contact tracing may give a more updated and complete picture of the actual number of household contacts of an infected individual. The rapid increasing incidence during the study period challenged the capacity of the contact tracing, causing the contact tracers to prioritize tracing of household contacts. This, as well as lacking a proper variable in the data for relationship between the primary case and contacts, became the reason our study only focus on household transmission. The resulting data set of household contacts is a rather heterogeneous group of individuals when it comes to age and number of vaccine doses and time since vaccination for the different age groups. This was not adjusted for in our analyses and the results should therefore be interpreted with caution.
Overall, our results are in line with other studies from both Norway [2], Denmark [3] and the UK [4]. The higher overall household SAR of Omicron seems to be due to a combination of higher intrinsic transmissibility and lower vaccine effectiveness. Three vaccine doses for contacts seems to decrease the risk of infection for both Delta and Omicron, but three doses seems to have limited effect of preventing transmission from vaccinated primary case in Omicron households.
References
- Emergency preparedness register for COVID-19 (Beredt C19). Norwegian Institute of Public Health. [Online] https://www.fhi.no/en/id/infectiousdiseases/coronavirus/emergency-preparedness-register-for-covid-19/.
- S. B. Jørgensen, K. Nygård, O. Kacelnik, et al. Secondary Attack Rates for Omicron and Delta Variants of SARS-CoV-2 in Norwegian Households. JAMA. 327(16):1610-1611, (2022). doi: 10.1001/jama.2022.3780
- F. P. Lyngse, L. H. Mortensen, M. J. Denwood, L. E. Christiansen, C. H. Møller, R. L. Skov, et al. SARS-CoV-2 Omicron VOC Transmission in Danish Households. medRxiv. (2021) https://doi.org/10.1101/2022.01.28.22270044
- SARS-CoV-2 variants of concern and variants ounder investigation in England. UK Health Security Agency. 2021.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Tumor Microenvironment Crosstalk and Therapeutic Implications
Publishing Model: Hybrid
Deadline: Nov 02, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in