The ALLAN-trial
Published in Cancer, General & Internal Medicine, and Pharmacy & Pharmacology
Introduction
The primary objective of palliative care is to enhance the quality of life (QoL) for patients facing life-threatening illnesses, with a particular emphasis on those with advanced cancer. Previous studies have shown promising results on QoL in patients with various cancer diagnoses when specialised palliative care (SPC) was integrated early (Haun et al. Cochrane Database of Systematic Reviews 2017). Despite growing enthusiasm for early palliative care, the optimal model for early SPC has yet to be determined. Hence, we aimed to conduct a randomized study in the Swedish setting to investigate the impact of early integration of SPC in patients with advanced gastrointestinal cancer. Our study is a collaboration between the Department of Oncology, Skane University Hospital and the Department of Palliative Care and Advanced Home Health Care , Skane, Sweden.
Method
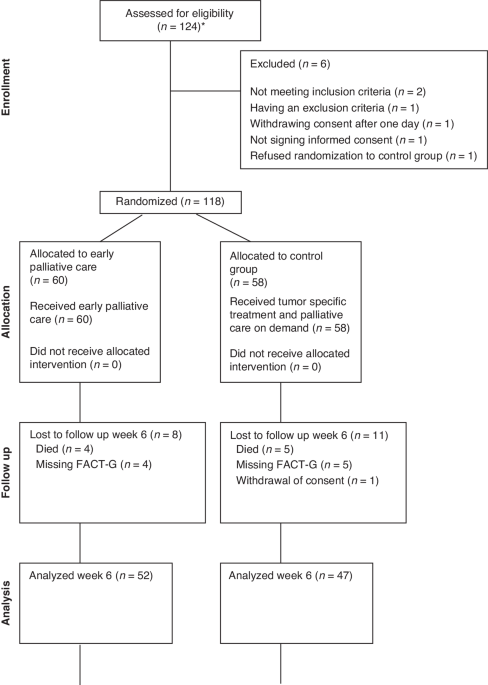
Our study included patients between December 2014 and April 2021. Patients with upper GI cancer (esophageal, gastric, hepatobiliary, and pancreatic cancer) eligible for first-line palliative chemotherapy and patients with lower GI cancer (colorectal cancer) eligible for second-line palliative chemotherapy were invited to this nonblinded randomized controlled trial.
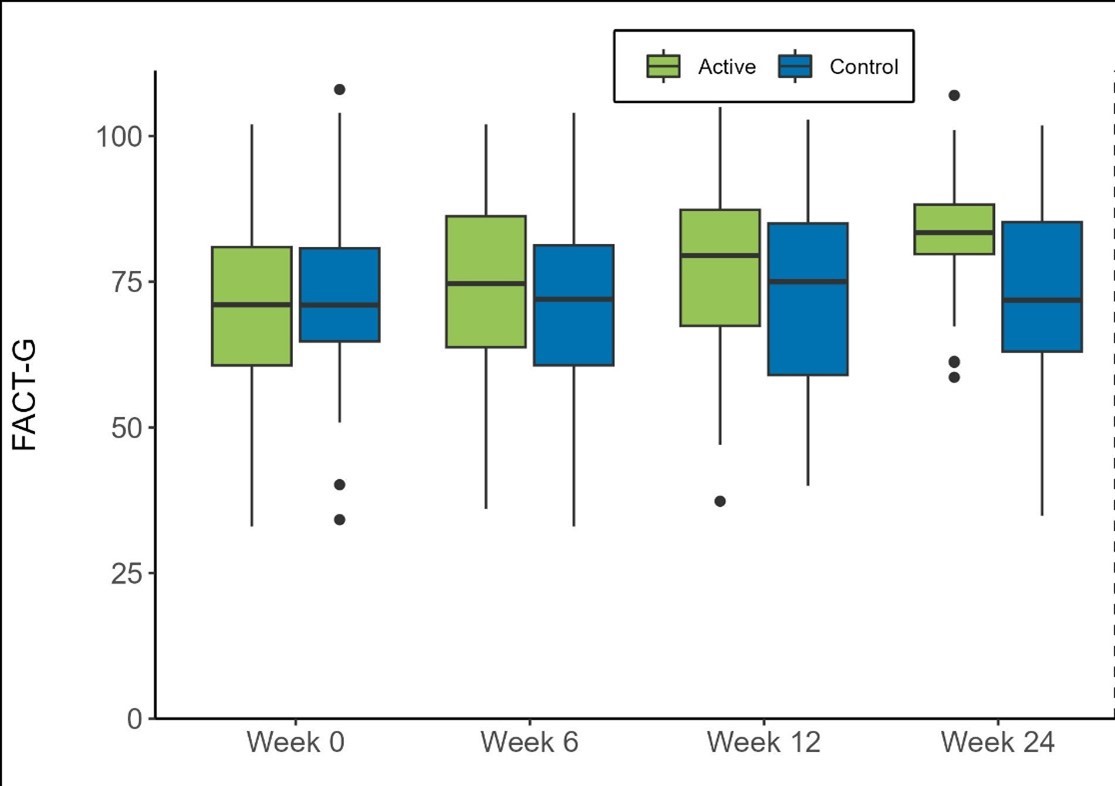
Quality of life was evaluated using the Functional Assessment of Cancer Therapy-General (FACT-G) questionnaire. This questionnaire measures health-related QoL in four dimensions: physical, functional, emotional, and social well-being over the past week. A higher FACT-G score indicates better QoL.
Intervention
All healthcare professionals should have skills to provide general palliative care for chronically ill patients, while SPC manages complex patients that require a multidisciplinary team. The SPC team consists of doctors and nurses specialised in palliative care. In addition, patients and their caregivers have access to dieticians, physiotherapists, and counselors. The care is home-based, and the intensity of home visits depends on the patient's individual needs and symptom burden. Patients in the active study group received their planned tumor-specific treatment at the outpatient clinic in the Department of Oncology. Additionally, a specialist palliative care physician and a palliative care nurse assessed them at their homes within six weeks following randomization. In reality, this meeting took place within a week of being included in the active arm of the trial. Admittance to inpatient care at the SPC ward could be arranged, generally for a shorter period, for symptom management and to allow respite for caregivers at home.
The control group was randomized to a standard of care arm in which SPC is initiated on demand by the treating oncologist or by the patient. All medical care, including SPC, was financed within the social security system.
Results
A total of 118 patients were randomized, and 60 were allotted early integration of SPC. The most common cancer diagnosis in the study cohort was pancreatic cancer (56%), hepatobiliary cancer (21%), and gastric cancer (9%). Quality of life was assessed at baseline and every sixth week. The median time of enrollment in SPC was 167 days for the active group and 39 days for the control group. All except eight patients (14%) of the control group were enrolled in SPC before death.
When looking at the mean total change in FACT-G score compared to baseline, the difference in this change between patients assigned to early integration of SPC and controls was 5.2 points (95% CI: -0.1–10.5, p=0.216) at week 6, 6.7 points (95% CI: 0.2–13.3, p=0.172) at week 12, and 13 points (95% CI: 5.7–20.2, p=0.004) at week 24, with all numerical differences in favor of the early-integration group. We found no differences in overall survival between the study groups.
Discussion
We observed improved QoL for patients with advanced gastrointestinal cancers when home-based SPC was introduced early and integrated with tumor-specific treatment. At 24 weeks after randomization, the increase in QoL was statistically significant, even though most patients in the control group also received SPC at some point during the study. The gain in mean total FACT-G scores, with a difference of 13 points between the groups at week 24, can be regarded as clinically meaningful, far exceeding the minimal important difference of 4–7 points.
In the present study, we measured QoL every 6 weeks to explore the hypothesis that a longer time of enrollment in SPC would correlate with the improvement in QoL compared to baseline. This approach weakened our statistical power as all p-values had to be adjusted to four analyses and hence multiplied by four. Even though we do not have statistically significant improvements in QoL at weeks 6 and 12, we argue that time enrolled in SPC matters. This argument is supported by the provided box plot (background picture), where the green box, representing the active group, climbs higher in QoL at each assessment.
We believe that the longer time of enrollment in SPC allows for a thorough work-up with early detection and treatment of cancer- and treatment-related symptoms, clear communication with caregivers and family, maintenance of QoL, and meaningful end-of-life discussion. The prognosis for these patients is dismal, and healthcare professionals and patients often overestimate the remaining time in life. If time from enrollment to death is short, the care must focus on symptom control and end-of-life care.
Conclusion
This prospective randomized trial of home-based PC strengthens the argument for early integration of SPC with tumor-specific treatment in patients with advanced gastrointestinal cancers. We found an improved QoL for patients with advanced gastrointestinal cancer 24 weeks after randomization to early integration of SPC.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in