Untangling the Complex Relationship Between Water Contact and Schistosome Infection: Insights from the SchistoTrack study in Uganda
Published in Earth & Environment, Ecology & Evolution, and Microbiology

Schistosomiasis is a neglected tropical disease that affects over 240 million people globally, mostly in sub-Saharan Africa. Populations living close to freshwater bodies such as rivers and lakes are most at risk. Human water contact through activities such as fishing, swimming or washing clothes, enables the schistosome parasite to bore through the skin and establish an infection. Currently, mass drug administration (MDA) using praziquantel is the mainstay strategy for schistosomiasis control, endorsed by the World Health Organization. MDA has made significant progress in reducing infection prevalence in school-age children across sub-Saharan Africa. However, in Uganda for instance, overall prevalence in infection rebounded despite repeated MDA1 as the treatment does not prevent reinfection. This illustrates that MDA alone is likely insufficient to sustain long-term reductions in infection prevalence. Complementary interventions such as behaviour change and water, sanitation, and hygiene (WASH) are critical for achieving elimination of schistosomiasis as a public health problem.
A focus on water contact behaviour
In schistosomiasis-endemic areas, water contact is typically pervasive; children may engage in recreational swimming, women in washing laundry and men in fishing or other occupational activities. Infection prevalence can remain stubbornly high in communities with high water contact levels. We focused on water contact behaviour within the SchistoTrack study across 38 communities in Western and Eastern Uganda. This study is a collaboration between Oxford University and the Uganda Ministry of Health. In SchistoTrack, the baseline prevalence across all ages 5-90 was 43% despite 13 or more rounds of MDA. Among participants, 47% reported to typically engage in one or more water contact activities per week. Yet not all water contacts are created equal in terms of infection risk; for example, swimming has higher bodily immersion than other activities and fishing can create a very long duration exposure. But even short activities can pose considerable risk if they are done midday when the parasite is most active. Identifying how the composition of water contact varies over age and gender, and identifying the individual, household, and village/environmental drivers of water contact could help to better identify at risk-groups of water contact. This could inform design of future exposure reduction interventions, especially as a recent study which conducted participatory mapping identified exposure reduction as a key local priority for schistosomiasis control in Uganda2.
A data-driven, comprehensive approach
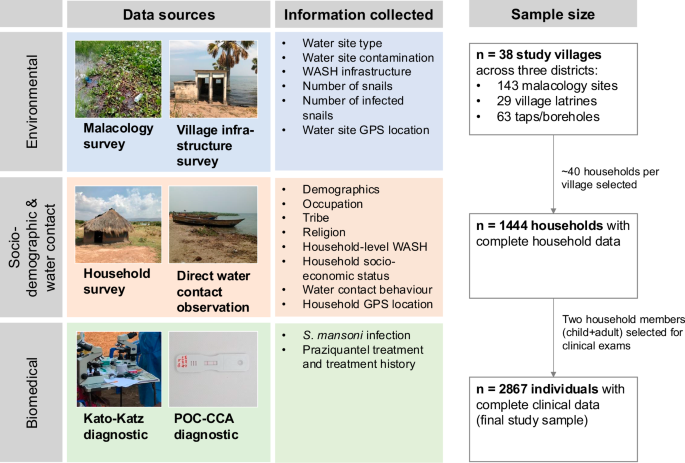
In this study, we combined household and clinical data on 2867 individuals with detailed village-level infrastructure and environmental data. We used Bayesian variable selection on a candidate set of 27 variables covering socio-demographics, biomedical factors, water, sanitation and hygiene, and environmental variables, and identified key determinants of water contact and infection separately. This enabled us to understand which types of factors and levels were relevant for water contact and how this differed from the determinants of infection. We also validated self-reported water contact data by triangulating survey responses with direct water contact observation data that were collected concurrently with the household surveys.
Water contact does not directly translate into infection
Our analysis revealed that current water contact of an individual was not strongly associated with current schistosome infection. We found distinct age-specific patterns of water contact and schistosome infection, with infection prevalence peaking at age 15, while water contact peaked much later, at age 30. We also found no significant positive relationship between village-level infection prevalence and water contact. Individuals in hotspot villages with infection prevalences exceeding 50% were not more likely to engage in water contact than individuals in lower prevalence villages (10-50%), challenging the assumption that hotspot villages were characterised by more intense water contact.
The interrelatedness of age and gender
While age and gender have often been considered separately, we found that the influence of gender on water contact patterns was highly age-dependent. Among children, males and females had similar water contact patterns, dominated by helping with household domestic activities, such as fetching drinking water or doing laundry. After age 15, males started to engage primarily in occupational water contact such as fishing and agriculture, and domestic water contact became an unimportant source of exposure. Females, by contrast, maintained high levels of domestic water contact throughout adulthood. Regression analysis supported the conclusion that gender differences in water contact among adults were mostly driven by differences in occupational and domestic water contact as males had lower water contact after occupation was accounted for.
The role of environmental factors
Environmental features also play a critical role in shaping water contact patterns. We showed descriptively that 80% of all individuals with water contact lived within just 0.34 km of lakes or rivers. For every 100m increase in household distance to waterbodies, the proportion of individuals with water contact decreased by 3.4%-points. Using regression analysis, we showed that the number of available water sites, the type of water site (beach, swamp, river, lake), and faecal contamination influenced individuals’ water contact behaviour. At the same time, abundance of infected snails, the intermediate hosts of the parasites, is not easily observable and thus, as expected, did not influence water contact patterns.
What does this mean for schistosomiasis control?
Our findings offer important insights for research and implementation of schistosomiasis control programs in Uganda and beyond. We emphasise that even though water contact was not associated with infection, this does not mean water contact is unimportant for infection as all infections are caused by water contact with infested freshwater at some point. The low correlation however suggests a potentially very significant role of immunity in infection which may be acquired through past exposure. Our study also shows that surveys provide a cost-effective and reliable way to assess water contact patterns at the population level. For national control programmes, collecting age, gender, and occupation information allows for a simple way of capturing key proxy indicators of water contact to profile groups at high exposure risk. We confirm the need to focus MDA on school-age children due to the high prevalence in this group despite low levels of water contact. The high concentration of water contact near waterbodies suggests opportunities for spatially targeted exposure reduction interventions. Our study underscores the need for improved tools to measure water contact. Developing standardized methods for collecting water contact data, as part of national monitoring and control programs, could help refine treatment frequency guidelines and enhance the effectiveness of schistosomiasis control strategies and monitoring efforts to track progress. There is also a need for future research using wearable GPS loggers to capture the role of human mobility and water site usage patterns, which would enable the integration of detailed water contact and environmental risk information to create indices of exposure.
References
- Deol, A. K. et al. Schistosomiasis — Assessing Progress toward the 2020 and 2025 Global Goals. N. Engl. J. Med. 381, 2519–2528 (2019).
- Fergus, C. A. et al. Shifting the dynamics: implementation of locally driven, mixed-methods modelling to inform schistosomiasis control and elimination activities. BMJ Glob. Health 7, e007113 (2022).
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Tumor Microenvironment Crosstalk and Therapeutic Implications
Publishing Model: Hybrid
Deadline: Nov 02, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in