Using deep learning to integrate diverse data for survival analysis in the critically ill
Published in Healthcare & Nursing

Critical care at intensive care units (ICU) spawn loads of detailed phenotypic data, and the pathophysiological status of patients may (and sometimes does) change quickly. This mix of vast data and clinical dynamicity requires swift yet well-informed decisions, often on the basis of overwhelming amounts of information.
Over the past 40 years, many ICU prognostic scores have emerged to facilitate bedside assessment of disease severity and mortality risk.1–4 Most scores in use in clinical settings, however, are based on simple regression methods with few routinely measured variables. Many models, further, provide only one-off static scores that fail to leverage and integrate prior disease history and the rich longitudinal data produced (and collected) as a by-product of critical care. Thus, prognostic models of the future should natively handle this multiverse of ICU data:
- Highly granular time-series/waveform data from, e.g., continuous electrocardiograms and continuous drug administration with infusion pumps;
- Static data such as prior disease history and demographics; and,
- Free text documenting pertinent clinical observations in an unstructured fashion.
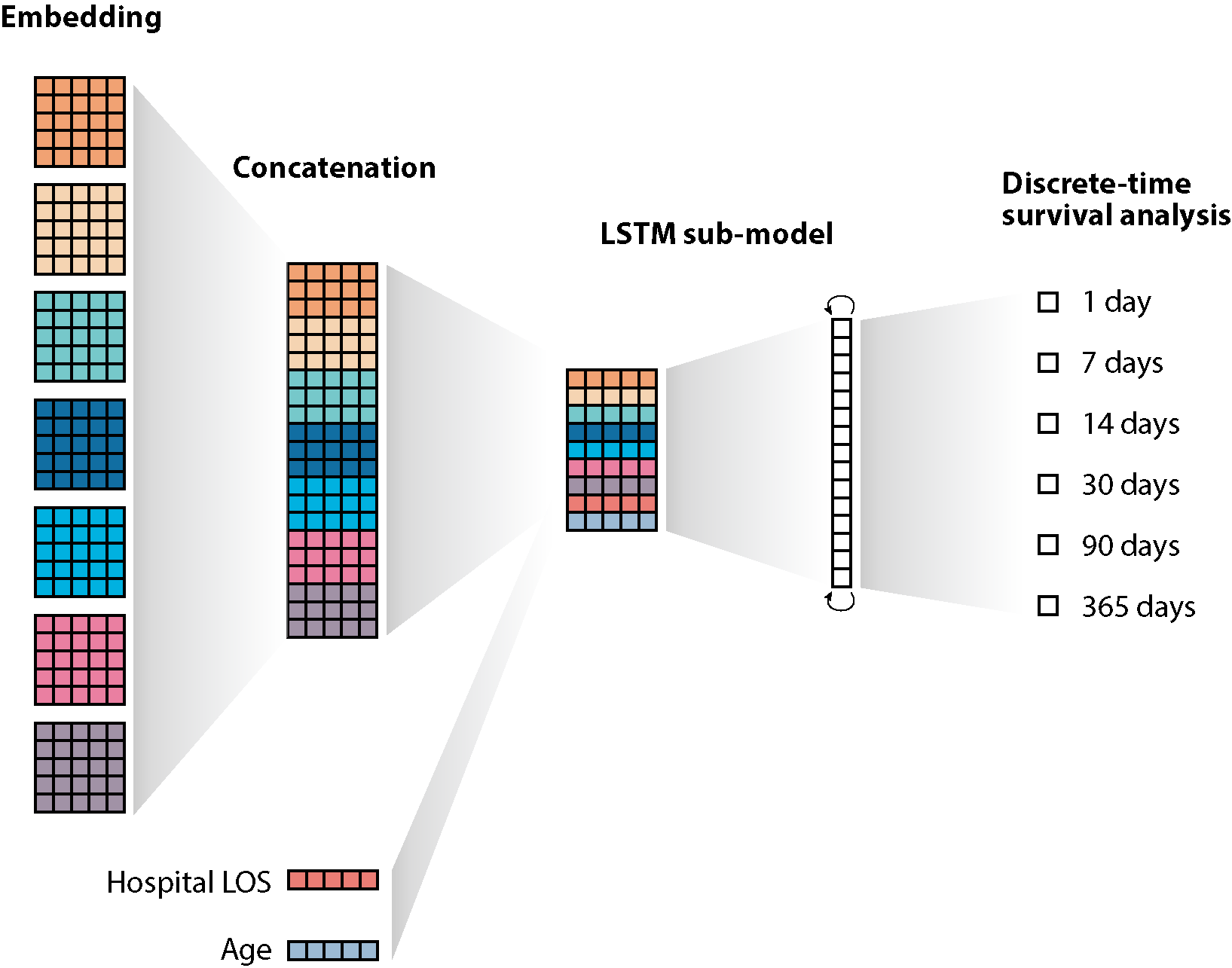
Hitherto, most severity scores have used static outcomes such as mortality risk (e.g. before discharge from the ICU or within 90 days).5 Such outcomes turn a continuous outcome into whether the patient is likely to pass away before or after an arbitrary date, yielding neat but problematic binary classification problems.6 Modelling the survival profile directly, on the other hand, may resolve these shortcomings. Particularly, the full survival profile is often of greater clinical interest than when using arbitrary thresholds for patient-level prognostication (but also for organisational planning). Further, the changing nature of the cohort is built into the discrete-time survival model, and model explanation techniques enable quantification and visualisation of the drivers of the predictions at short, mid and long term.
To address these issues, we trained a machine learning model on data from patients admitted to ten Danish ICUs between 2011 and 2018. We used a novel technique for using "all kinds of data" as inputs, by casting all input data (structured and unstructured alike) into text strings, embedding them into a dense representation, and using these dense representations as input in a recurrent neural network with a multi-label output layer representing the chance of survival for a range of different follow-up time windows. This modular approach has several advantages: feature engineering and data pre-processing efforts are substantially minimised, the model learns important trends by itself, and very different data types natively flow into the model as inputs.
The deep learning models outperformed traditional Cox proportional-hazard models with concordance index in the ranges 0.72-0.73, 0.71-0.72, 0.71, and 0.69-0.70, for models applied at baseline and 24, 48, and 72 hours after ICU admission, respectively. Calibration was best for doorstep models; the tendency of predictions in the mid-range time points to be slightly pessimistic is likely amenable to recalibration with prospective data. Not surprisingly, age at admission was a key driver throughout.
In conclusion, our recent paper in npj Digital Medicine presents an explainable deep learning model that provides personalised predicted survival profiles for ICU patients. The model incorporates all available data without data cleaning and modest pre-processing.
This work was funded by the Novo Nordisk Foundation (Grant agreement NNF14CC0001) and the Innovation Fund Denmark (Grant agreement 5153-00002B).
References
- Glance, L. G., Osler, T. M. & Dick, A. W. Identifying quality outliers in a large, multiple-institution database by using customized versions of the Simplified Acute Physiology Score II and the Mortality Probability Model II0. Crit. Care Med. 30, 1995–2002 (2002).
- Knaus, W. A. et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 100, 1619–36 (1991).
- Vincent, J. L. et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on ‘sepsis-related problems’ of the European Society of Intensive Care Medicine. Crit. Care Med. 26, 1793–800 (1998).
- Lemeshow, S. et al. Mortality Probability Models (MPM II) based on an international cohort of intensive care unit patients. JAMA 270, 2478–86 (1993).
- Zimmerman, J. E., Draper, E. A. & Wagner, D. P. Comparing ICU Populations: Background and Current Methods. in Evaluating Critical Care 121–139 (Springer Berlin Heidelberg, 2002). doi:10.1007/978-3-642-56719-3_9
- Courtland, R. Bias detectives: The researchers striving to make algorithms fair news-feature. Nature 558, 357–360 (2018).
Follow the Topic
-
npj Digital Medicine
An online open-access journal dedicated to publishing research in all aspects of digital medicine, including the clinical application and implementation of digital and mobile technologies, virtual healthcare, and novel applications of artificial intelligence and informatics.

Related Collections
With Collections, you can get published faster and increase your visibility.
Digital Biomarkers for Enabling Proactive Clinical Decisions
Publishing Model: Open Access
Deadline: May 18, 2027
Impact of Agentic AI on Care Delivery
Publishing Model: Open Access
Deadline: Jul 12, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in