Valuing Lived Experience: Building the Evidence for Better Care in Pernicious Anaemia
Published in Healthcare & Nursing, Social Sciences, and General & Internal Medicine

The story behind the research
Pernicious anaemia (PA) is a lifelong autoimmune disease leading to severe B12 deficiency. Despite being manageable with regular treatment, it often remains under-recognised and inconsistently managed in clinical practice. This led to the James Lind Alliance Priority Setting Partnership uniting patients, carers, and clinicians to identify the most urgent unanswered questions. At the top of the list were how to improve diagnosis, to understand why symptoms often persist despite treatment, and to explore individual treatment needs.
Working in partnership with the Pernicious Anaemia Society (PAS) and the University of Surrey, and in collaboration with national and international experts, we aimed to turn lived experience into research. Using insights shared by people with PA through PAS, we co-designed a large-scale survey to capture real-world patterns in diagnosis, testing, treatment, and co-existing conditions.
Through PAS, hundreds of people had already described years of unexplained symptoms, repeated misdiagnoses, and ongoing struggles even after diagnosis, as symptoms returned between injections and treatment differed from one practice to the next.
Key findings
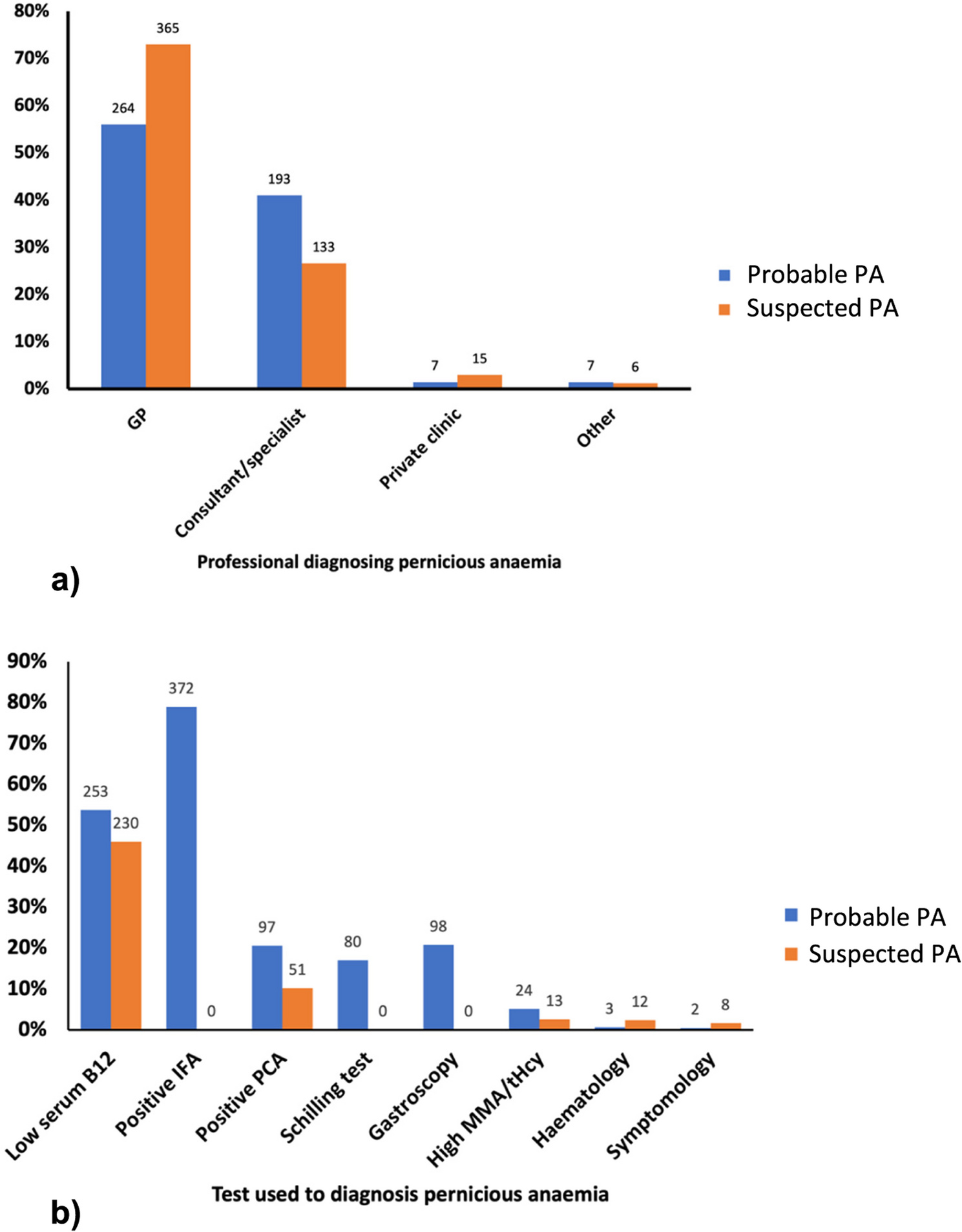
- Diagnosis is delayed. More than one in three people waited at least three years to receive a diagnosis, and one in four waited five years or longer.
- Testing was inconsistent. Only 38% had ever been tested for the key biomarker intrinsic factor antibodies.
- Treatment is variable. Just over half reported a need for more frequent injections than the recommended injections 2-3 monthly schedule (as stated in the British National Formulary), supporting that the “one-size-fits-all” is not appropriate
- Comorbidities were common. About one-third had another autoimmune disease, such as autoimmune thyroid disease or vitiligo. Around 40% also reported iron deficiency.
- Family patterns emerged. Nearly one-third had at least one other family member with PA, and nearly 50% had family members with another autoimmune condition.
These findings highlight that PA presents in diverse ways and cannot be managed through a single diagnostic or treatment pathways.
Why does it matter?
For clinicians, our findings highlight the need to revisit how PA is diagnosed and managed. Early recognition, appropriate testing, and flexible treatment intervals could make a real difference to patient wellbeing.
For people living with PA, the study validates lived experience. It confirms that delayed diagnosis and fluctuating symptoms are not isolated cases, but rather systemic challenges. It also highlights the need for improved life-long therapy and management protocols.
For researchers, the dataset provides a foundation for future research, supporting studies on genetics, multi-morbidity, and studies on symptom trajectories that can help move towards more precision medicine-based care.
This study also shows the power of partnership between researchers and people with lived experience, whose insights shaped every stage of the project, from survey design to interpretation of the results.
What comes next...
This study represents the first step in a wider research programme shaped by the James Lind Alliance priorities. Ongoing projects are now exploring better ways to monitor symptoms using smart-watch technology and developing more precise, holistic and diverse treatment, management and follow-up approaches for people with pernicious anaemia.
Follow the Topic
-
BMC Primary Care
Previously known as BMC Family Practice, this is an open access, peer-reviewed journal that considers articles on all aspects of primary health care research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Sleep health and primary care
Sleep health is a critical yet often overlooked aspect of overall well-being, particularly in the context of primary care. Sleep disorders, including insomnia and obstructive sleep apnea, can significantly impact patients' physical and mental health, leading to complications that may complicate primary care management. Sleep issues are becoming increasingly recognized for their chronicity, widespread prevalence, and influence on other chronic conditions. Therefore, understanding the relationship between sleep health and primary care practices is vital. This Collection aims to explore the intersection of sleep health and primary care, shedding light on innovative approaches to assessment and treatment.
Continued exploration in this area could pave the way for groundbreaking advancements in the management of sleep health care within primary care settings. As more research is conducted, we may see innovative approaches to screening and treating sleep disorders that can assist primary care providers in addressing these issues more effectively and efficiently. Future studies may also illuminate the impact of sleep health on chronic disease prevention and management, ultimately leading to a more holistic approach to patient care. By enhancing sleep health awareness among primary care providers, we can promote comprehensive care that acknowledges the crucial role of sleep.
We invite submissions on a range of topics that include, but are not limited to:
- Management of insomnia in primary care
- Management of obstructive sleep apnea in primary care
- The intersection between sleep disturbances and chronic disease
- Integrated behavioral health approaches to the management of sleep disorders
- Screening tools for sleep disorders in primary care
- Implementation of new models of care for sleep disorders
This Collection supports and amplifies research related to SDG 3: Good Health and Well-being.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 07, 2027
Ethics and regulation of AI in primary care
The integration of artificial intelligence (AI) into primary care is rapidly transforming healthcare delivery, enabling more personalized, efficient, and effective patient care. However, the ethical and regulatory challenges associated with the deployment of AI technologies in this context are multifaceted and require thorough examination. Issues such as patient privacy, data protection, informed consent, and the potential for algorithmic bias are at the forefront of discussions surrounding AI's role in healthcare. As AI systems increasingly influence clinical decision-making, understanding the ethical frameworks and regulatory requirements governing their use is essential for safeguarding patient rights and ensuring equitable access to healthcare services.
The significance of addressing the ethical and regulatory dimensions of AI in primary care lies in its potential to enhance patient trust and ensure that AI applications are developed and implemented responsibly. Recent advancements in AI have demonstrated its capabilities in improving diagnostic accuracy and streamlining administrative tasks; however, these benefits must be balanced with robust protections for patient data and ethical considerations regarding decision-making. Furthermore, the lack of comprehensive regulations can lead to inconsistencies in AI application and misuse, which could undermine public confidence in these technologies.
In this Collection, we welcome submissions that span a wide array of topics, including but not limited to:
- Ethical considerations in AI applications
- Data protection and patient privacy in AI
- Informed consent processes for AI use
- Regulatory frameworks for AI in primary care
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 28, 2027


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in