SARS-CoV-2 variants of concern and possible future waves of infection
Published in Healthcare & Nursing
Background
When a new pathogen emerges and becomes established in the human population, there is initially large uncertainty about its virological properties, the epidemiological characteristics of the disease it inflicts and how best to tackle its spread. Our ideas and understanding change as new information comes to light during the outbreak.
As SARS-CoV-2 mutates over time, we are in a continuing cycle to update our understanding. Mutations generate new variants of the virus, potentially altering transmissibility, severity and escape from natural or vaccine-derived immunity, which can be advantageous for the virus and be of increased concern to us. Such variants have been designated “Variants of Concern” (VOCs) [1]. At the time of writing, two of the most notable VOCs have been the Alpha and Delta variants.
There is a consensus that the Alpha variant has a substantial transmission advantage over prior variants, with estimates ranging between 40% and 80% more transmissible [2-6], and a higher mortality compared to prior variants at a population level [7-9]. The observed growth of the Delta variant in the UK relative to the Alpha variant suggests it has a substantial transmission advantage [10].
The number of countries reporting variants causing concern continues to rise [11]. We are in a race with the virus to mitigate the health harms it inflicts through generation of variants and further infection. This raises the following questions:
- What types of variants are of concern to public health?
- How do different types of VOCs behave at a population level?
- How quickly would an updated vaccine be required to have an effect on an emerging VOC?
How can we study the potential impact of VOCs with different types of transmission behaviour?
One way to investigate the epidemiological impact of a potential VOC would be to run a clinical trial seeding different populations with different VOCs and/or intervention strategies. But this would clearly be highly unethical, so how may we instead gather insight on our VOC questions of interest?
In our research we instead use mathematical models to analyse infectious disease dynamics. Models can give an estimated range of predicted possibilities, given the currently available evidence. We used modelling to investigate two mechanisms in which SARS-CoV-2 variants may be a public health concern: (i) being more transmissible than resident variants (those variants circulating in the community prior to the arrival of the VOC) and/or, (ii) evading immunity.
We took three VOCs as examples: (i) a VOC that was more transmissible than the existing resident variants in circulation (which we labelled “VOC MT”), (ii) a VOC that had partial immune escape to vaccination and prior infection but no transmission advantage (“VOC E”), and (iii) a VOC that had partial immune escape to vaccination and prior infection, but was less transmissible than the resident variants (“VOC LT+E”). We summarise these three example VOCs in Table 1.
Table 1: Transmissibility and immune escape properties for our example VOCs. “Relative transmissibility” is the transmission of the VOC relative to the resident variants. For the proportional vaccine efficacy measure, a value of 1 corresponds to the vaccine efficacy against the VOC being the same as the efficacy of the vaccine towards resident variants, while 0 would correspond to the vaccine offering zero protection against the VOC. For the proportional prior-infection efficacy measure, a value of 1 corresponds to previous infection by the resident variants giving complete protection against the VOC (and vice versa), with values less than 1 corresponding to previous resident variant infection providing imperfect cross-protection against the VOC (and vice versa).
|
Scenario |
Description |
Relative transmissibility |
Proportional vaccine efficacy |
Proportional prior-infection efficacy |
|
VOC MT |
More transmissible, no immune escape |
1.5 |
1 |
1 |
|
VOC E |
Equally transmissible, partial immune escape |
1 |
0.75 |
0.75 |
|
VOC LT+E |
Less transmissible, partial immune escape |
0.8 |
0.75 |
0.75 |
The effect of a VOC depends on the population immunity and the level of nonpharmaceutical interventions (NPIs). We set up our models to resemble the situation in England in May 2021.
Effects of potential VOCs on resultant waves of SARS-CoV-2 infection
We began with a simplified compartmental model that had no age-structure. The model grouped the population by infection status. We had four broad infection status groups (susceptible, latent, infectious, recovered). Our model considered resident variants with a small number of initial VOC infecteds introduced on 17th May 2021. We tracked the infection status for both the resident variant and the VOC separately as they co-circulated amongst the population.
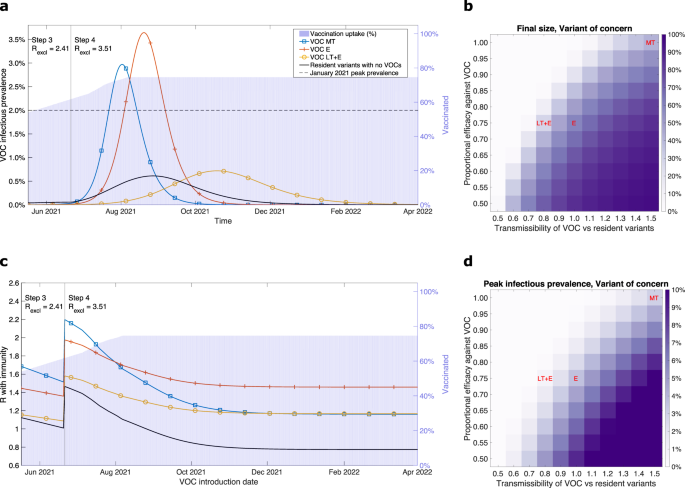
We found the epidemiological trajectories for example VOCs to be wide-ranging and reliant on their transmissibility and immune-escape capability. More transmissible VOCs (VOC MT) or VOCs with a degree of immune escape (VOC E) could generate a wave of infection whose peak exceeded the estimated peak prevalence during the January 2021 wave (Figure 1, blue and red lines). Meanwhile, a less-transmissible variant with partial immune escape (VOT LT+E) could be revealed as NPIs are lifted, causing an appreciable wave of infections (Figure 1, yellow line).
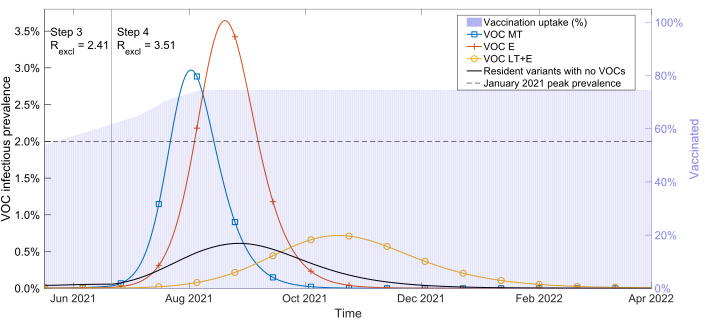
Figure 1: Using our simple SARS-CoV-2 transmission model, VOC infectious prevalence over time for our three example VOCs: more transmissible (VOC MT, blue line with square markers), equal transmissibility with immune escape (VOC E, orange line with plus sign markers), less transmissible with immune escape (VOC LT+E, yellow line with circle markers). We also show resident variants alone in the absence of any VOC being introduced (black line with no markers). We represent the vaccine uptake in the population through time via background shading. The vertical solid line was the earliest possible transition time into Step 4 of the relaxation roadmap in England (21st June 2021), resulting in a change in strength of nonpharmaceutical interventions.
Our first model was simplistic in that it only looked at infection and did not capture all known factors that impact SARS-CoV-2 infection and COVID-19 disease severity, such as age. Such a model can be useful, however, as it provides swift insight in the time-critical setting of a global public health emergency. We must find a balance between having a model of sufficient detail to provide reliable insights on the objective and the time required to obtain such insight. Sometimes getting an approximate answer quickly is more valuable than getting a more precise answer after the policy decision has already been taken [12]. Models with additional complexities typically require longer development times and finer-resolution data to be reliably parameterised [13].
To include reductions in the severity of cases due to vaccinations, however, we turned to a more complex compartmental model [14] that included age-structure and a broader range of clinical outcomes (hospitalisations and deaths, as well as infections).
We found a VOC with either a substantial transmission advantage over resident variants or immune escape could provoke a wave of hospitalisations in England comparable to those seen in January 2021 (Figure 2). Reassuringly, our results for our illustrative VOC scenarios using the age-structured model had similar patterns to outputs from the simple model.
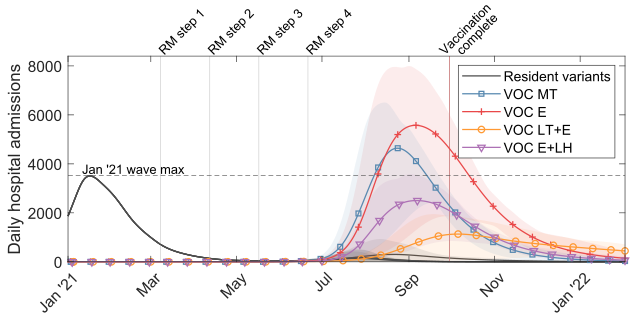
Figure 2: Using our age-structured SARS-CoV-2 transmission model, time series of estimated daily hospital admissions (thousands) for our example VOC scenarios. Solid lines show the mean at each timepoint and the shaded ribbons visually represent a range of predicted outcomes (95% prediction intervals). The vertical light red line corresponds to the projected date under our vaccine roll-out speed assumption where all those in the adult population (18+ years) in England who accept the vaccine would have received two doses. We also present an additional VOC, similar to VOC E, except with a lesser reduction in vaccine-derived efficacy against hospitalisation (VOC E+LH, purple, inverted triangle markers).
We focused here on VOCs that had either an advantage in terms of transmissibility or to escape previously acquired immunity (but not both). Within our paper we also carried out sensitivity analyses to consider VOCs possessing a combination of both advantages.
Introduction of VOCs and VOC-targeted vaccines
For our final piece of analysis we used stochastic modelling approaches to explore how the timing of the introduction of a presumptive VOC-targeted vaccine and the rate of VOC introductions into the population impact the trajectory of the epidemic.
We found that if VOC importations per day are sufficiently small, a VOC-targeted vaccine introduced early enough could have an appreciable effect on the outbreak by reducing the outbreak size and peak in infection. Conversely, if importations are not sufficiently controlled, it is possible for the VOC epidemic to be largely over by the time a VOC-targeted vaccine is deployed.
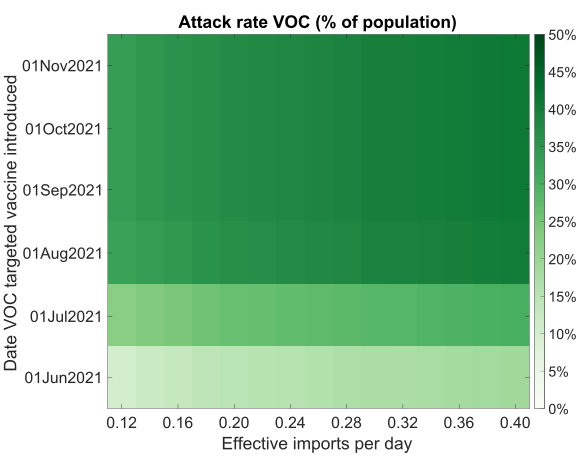
Figure 3: VOC outbreak final size for differing effective VOC importation counts and introduction date of a VOC targeted vaccine.
Does modelling give us all the answers?
We take a moment to emphasise the importance of interpreting findings from model-based studies by considering the assumptions made and deliberating anticipated implications under alternative scenarios. These reflections are required because the real world is always much more complex than can be represented in a model and chance will always play a role.
For example, our analyses would be affected by making different assumptions on the rollout speed of the vaccination programme, or the relaxation and/or strengthening of non-pharmaceutical interventions. In our models we also assumed no waning immunity and no seasonality. The presence of these factors would likely impact the timing of future waves of infection.
Implications of our modelling study
Overall, quickly assessing a substantial change in the risk of infection, morbidity and mortality posed by a new SARS-CoV-2 variant is tricky. There is not a simple relationship to describe the interactions between any novel variant, disease control policy, adherence to interventions and the historic patterns of infection and vaccination.
Nevertheless, countering the emergence and establishment of a problematic VOC requires rapid early detection and a swift public health response to extinguish infection clusters. Close monitoring of the evolution of SARS-CoV-2 across a range of geographical scales is needed to enhance local situational awareness and quantify risk from VOCs. In conjunction, mathematical models, matched to epidemic data, remain a contributory public health tool for both assessing new threats and for scoping potential dangers.
For further details, our full paper is available at: https://doi.org/10.1038/s41467-021-25915-7
References
[1] World Health Organization. Tracking SARS-CoV-2 variants (2021). URL https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/. [Online] (Accessed: 30 September 2021)
[2] Davies NG, Abbott S, Barnard RC, Jarvis CI, Kucharski AJ, et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. (2021) Science 372(6538):eabg3055. doi:10.1126/science.abg3055.
[3] Volz E, Mishra S, Chand M, Barrett JC, Johnson R, et al. Transmission of SARS-CoV-2 Lineage B.1.1.7 in England: Insights from linking epidemiological and genetic data. (2021) medRxiv. doi:10.1101/2020.12.30.20249034.
[4] Eales O, Page A, Tang SN, Walters CE, Wang H, et al. SARS-CoV-2 lineage dynamics in England from January to March 2021 inferred from representative community samples. (2021) medRxiv. doi:10.1101/2021.05.08.21256867.
[5] Vohringer HS, Sanderson T, Sinnott M, De Maio N, Nguyen T, et al. Genomic reconstruction of the SARS-CoV-2 epidemic across England from September 2020 to May 2021. (2021) medRxiv. doi:10.1101/2021.05.22.21257633.
[6] House T, Pellis L, Pouwels KB, Bacon S, Eidukas A, et al. Inferring Risks of Coronavirus Transmission from Community Household Data. (2021) ArXiv e-prints page arXiv:2104.04605
[7] Davies NG, Jarvis CI, Edmunds WJ, Jewell NP, Diaz-Ordaz K, et al. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. (2021) Nature 593(7858):270–274. doi:10.1038/s41586-021-03426-1.
[8] Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K,et al. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study. (2021) BMJ 372:n579. doi:10.1136/bmj.n579.
[9] Grint DJ, Wing K, Williamson E, McDonald HI, Bhaskaran K, et al. Case fatality risk of the SARS-CoV-2 variant of concern B.1.1.7 in England, 16 November to 5 February. (2021) Eurosurveillance 26(11):2100256. doi:10.2807/1560-7917.ES.2021.26.11.2100256.
[10] Challen R, Dyson L, Overton C, Guzman-Rincon L, Hill EM, et al. Early epidemiological signatures of novel SARS-CoV-2 variants: establishment of B.1.617.2 in England. (2021) medRxiv. doi:10.1101/2021.06.05.21258365.
[11] World Health Organization. Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update (2021). URL https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Online] (Accessed: 30 September 2021)
[12] Whitty CJM. What makes an academic paper useful for health policy? (2015) BMC Medicine 13:301. doi:10.1186/s12916-015-0544-8.
[13] Funk S, King AA. Choices and trade-offs in inference with infectious disease models. (2020) Epidemics 30:100383. doi:10.1016/j.epidem.2019.100383.
[14] Keeling MJ, Dyson L, Guyver-Fletcher G, Holmes A, Semple MG, et al. Fitting to the UK COVID-19 outbreak, short-term forecasts and estimating the reproductive number. (2020) medRxiv. doi:10.1101/2020.08.04.20163782.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Tumor Microenvironment Crosstalk and Therapeutic Implications
Publishing Model: Hybrid
Deadline: Nov 02, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in