A recurring theme in the treatment of patients with newly diagnosed multiple myeloma has been ‘more is more’. Triplet induction therapy led to better progression-free (PFS) and overall survival (OS) compared to doublet induction (as in the SWOG S0777 trial that established the superiority of bortezomib, lenalidomide, and dexamethasone). Early autologous stem cell transplant has been associated with a significant PFS benefit over a deferred-transplant strategy (as in the IFM-2009, DETERMINATION, and FORTE trials). The CASSIOPEIA and PERSEUS trials have shown that quadruplet induction therapy with an anti-CD38 monoclonal antibody is associated with deeper responses and superior PFS over triplet induction therapy. This has led to a renewal of the concept of ‘total therapy’, using all the most active anti-myeloma agents together, which was first popularized by the kitchen-sink approaches at the University of Arkansas for Medical Sciences that employed cytotoxic (and much more toxic) therapy combinations.
With the wealth of highly effective agents we now have to offer patients with newly diagnosed multiple myeloma, is conventional cytotoxic chemotherapy still necessary? High-dose melphalan followed by a stem cell rescue has persisted as a standard of care, but is it time to consider whether ‘less is more’ or at least ‘just as good’? Can stem cell transplant be eschewed for some patients? And if so, might extending induction therapy and/or maintenance therapy help to make up for forgoing transplant? We wanted to explore this concept further, incorporating the best of available induction therapy and measurable residual disease diagnostics.
In this phase II trial, we investigated the efficacy and safety of 24 cycles of daratumumab in combination with carfilzomib, lenalidomide, and dexamethasone (Dara-KRd) without transplant among patients with newly diagnosed multiple myeloma (regardless of transplant eligibility). Patients received 8 induction cycles of Dara-KRd with twice-weekly carfilzomib, and they had the option to harvest stem cells after 4-6 cycles of protocol therapy to permit a stem cell transplant in the future. Patients then proceeded with 16 additional cycles of Dara-KRd as extended consolidation/maintenance to complete 24 cycles in total, after which patients and investigators were recommended to choose a maintenance therapy (single-agent lenalidomide was recommended).
The primary endpoint of this trial was the rate of stringent complete response (sCR) and/or measurable residual disease (MRD) negativity < 10-5 at the end of cycle 8 (C8). This was done to account for patients non-evaluable for MRD by next generation sequencing (NGS) due to unavailable or untrackable clonal sequences along with the limitation of accurately distinguishing the IgG kappa monoclonal antibody daratumumab from IgG Kappa paraprotein on immunofixation. MRD was also assessed on peripheral blood samples using mass spectrometry with the EXENT system and liquid chromatography mass spectrometry (LC-MS).
A total of 42 patients were treated, 40 of whom were evaluable for the primary endpoint. The rate of sCR and/or MRD<10-5 following C8 was 75%, thereby meeting the statistical threshold for efficacy. As for the key secondary endpoints, the 10-6 MRD negative rate was only 35% after C8 but improved to 53% as best response with longer treatment. Agreement between EXENT and NGS was high and increased over time; agreement between LC-MS and NGS was lower. The estimated 3-year PFS was 85%: 100% for standard-risk disease, 92% for patients with 1 high-risk cytogenetic abnormality (HRCA), and 60% for 2+ HRCA. Of the 7 patients with progression, 6 had at least one of the following: extramedullary disease (n=4), 2+ HRCA (n=4), or circulating plasma cells (n=1). Using the landmark method, neither C8 MRD status by NGS, EXENT nor LC-MS were associated with PFS. However, EXENT negative status as best response was associated with superior PFS and none of the patients with LC-MS negativity experienced disease progression. Importantly, none of the 11 patients with sustained MRD < 10-5 had disease progression. The estimated 3-year OS was 95% and there were no treatment-related deaths.
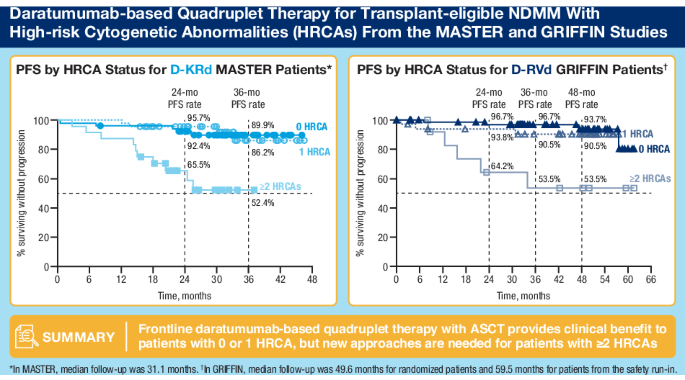
What can be made of these results from a nonrandomized study of extended Dara-KRd without transplant in newly diagnosed myeloma? First, the MRD negativity rates compare favorably with other quadruplet induction + transplant approaches, though it appears that achieving MRD negativity at the 10-6 threshold may take longer when transplant is deferred. Perhaps more impressive is that the estimated 3-year PFS among patients with no high-risk features was 100% and was 92% even for those with 1 HRCA. This suggests that quadruplets – with or without transplant – can lead to excellent outcomes and may be changing the way that we think about what constitutes high-risk disease. Harboring a single HRCA may not portend poor outcomes any longer! Identifying the optimal treatment for patients with 2+ HRCA remains a challenge. The 3-year PFS of 60% in this study leaves much to be desired, though this is on par with what has been seen with quadruplets and transplant. The current treatment approach for patients with 2+ HRCA is unsatisfactory, regardless of transplant; it is our hope that earlier use of chimeric antigen receptor (CAR) T-cell therapy and/or bispecific antibodies may help to change the treatment paradigm!
This study is the first to show that extended Dara-KRd can induce and sustain deep and durable responses without the use of transplant and provides a signal of efficacy in a population that is typically recommended to proceed with early transplant. The phase III CEPHEUS and IMROZ studies studying Dara-VRd and Isatuximab-VRd, respectively, as frontline approaches in transplant-deferred settings may help to further inform on transplant-free approaches to newly diagnosed multiple myeloma. However, we will still need randomized studies to answer whether transplant can be bypassed in favor of extended quadruplet treatment. Even if transplant can be avoided, the optimal duration of quadruplet therapy will remain an ongoing question before we can truly say ‘less is just as good’.
Follow the Topic
-
Blood Cancer Journal
This journal seeks to publish articles of the highest quality related to hematologic malignancies and related disorders.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in