Implementation Strategies in Suicide Prevention
Published in Healthcare & Nursing, Social Sciences, and Sustainability

Note: The views expressed in this blog poster are those of the author and do not necessarily reflect the position or policy of the U.S. Department of Veterans Affairs or the United States government.
We say often that the “how” of suicide prevention is just as important as the “what”. Many intervention and prevention programs have been developed that are promising for reducing suicide risk, but it can be difficult for them to spread due to a variety of challenges such as gaps in training and logistical support. The goal of our review was to understand how the broader field has utilized implementation strategies for supporting suicide prevention interventions and programs. I strongly believe that we heal in community and that we also learn in community. Understanding strategies used by the field allows us to all grow together to ensure our interventions and programs reach those in need.
You might be wondering what implementation science is exactly and what are implementation strategies. Implementation strategies are strategies used to support a system in using a given intervention or program. Implementation science can be jargony, so I will share an example using one of my favorite foods, pizza. Imagine a local pizzeria wanted to start making a new kind of pizza that required more time to bake and different ingredients. Things that could come up include how much the new kind of pizza would add to the current menu, the degree to which ingredients are available and cost-effective, and if they had enough staff to support the process. In addition, it may be unclear whether the community wants this new kind of pizza or would prefer something different. Implementation science works to address these questions so that the pizza or a suicide prevention program can reach the end user. My team and I worked to identify what types of implementation strategies are currently in use as well as gaps in the literature. Our original goal was to understand how use of specific strategies is associated with successfully deploying interventions. Unfortunately, the state of the literature was not yet there for us to do so, as many papers did not clearly document their implementation processes and outcomes. There remains a strong need for sharing detailed experiences of implementing suicide prevention programs so we can build upon this collective wisdom.
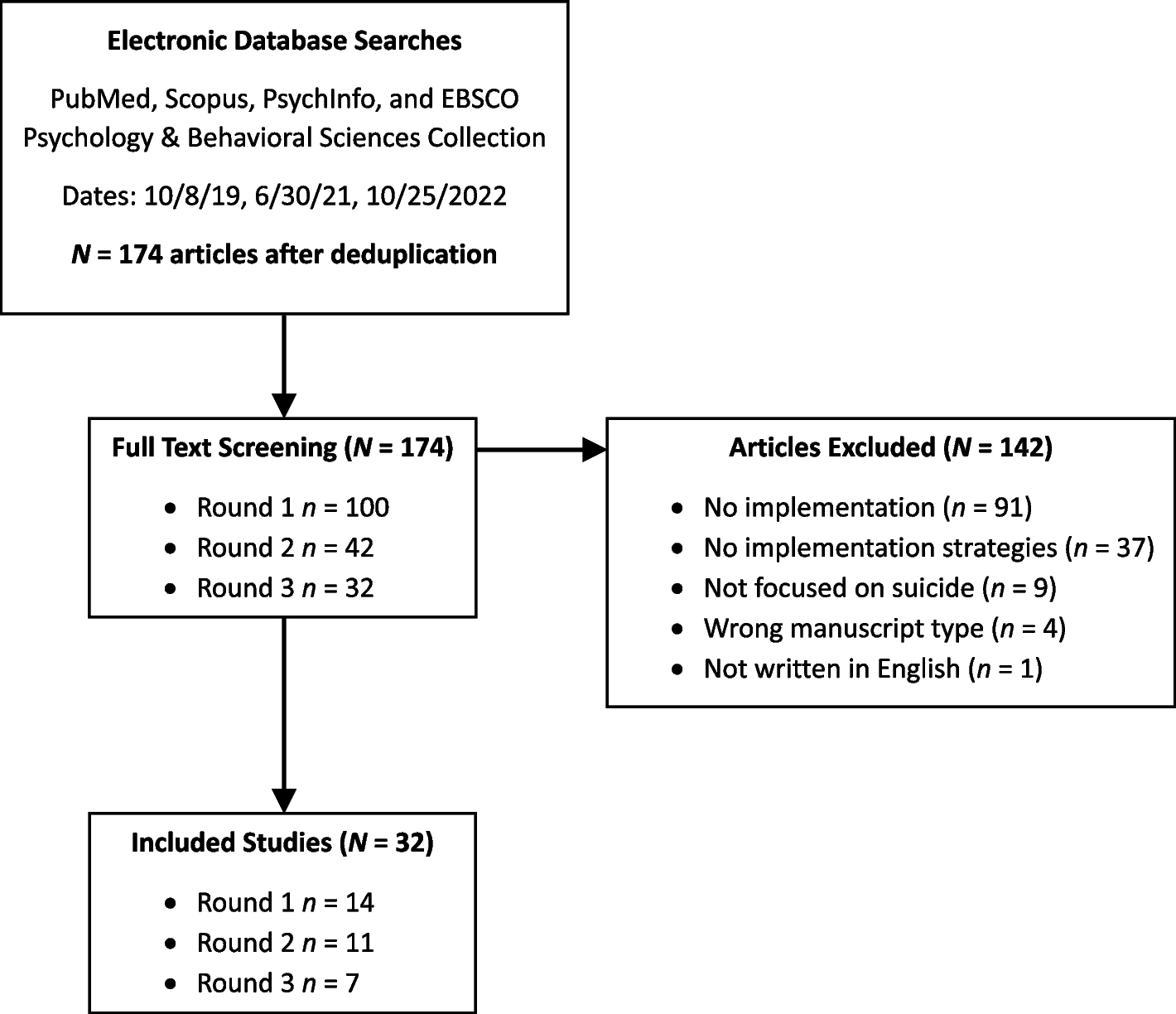
As we think about the “how” of things, the work for this review occurred over several years with initial challenges with making sure we were capturing all the literature we could. It was both exciting and work-intensive to see the literature grow rapidly, as we did several rounds of gathering articles for our review. Once we started documenting the implementation strategies being used, it became clear that we needed to find some way to organize them, as the coding systems from the broader literature had dozens and dozens of strategies. We found that training and education-based strategies as well as iterative refinement (e.g., evaluating and revising interventions based on field experience) were the most commonly used across the field. This makes sense as increasing suicide prevention skills and systematically evaluating and optimizing an intervention are important for making a given intervention successful in a given setting. However, fewer studies worked to support clinicians and engage those who would use the intervention. Active engagement is important for ensuring that the interventions we make can be used effectively and respond to the needs of our communities.
Although we couldn’t clearly identify which implementation strategies work best, the hope is our review can encourage the field to share the work being done at a level where we can build upon our successes and challenges. For this year’s Suicide Prevention Month, I encourage you to take a moment for whatever you are doing to support suicide prevention and reflect on the “how”. That moment could help make sure that the next person in crisis is able to get to the support they need. In many ways, the multiple pieces needed for a positive experience happen long before the person even makes the call. Implementation science provides a way for those pieces to be assembled into a coherent puzzle to ensure all those at-risk for suicide get connected to care.
Follow the Topic
-
Implementation Science
This journal publishes research relevant to the scientific study of methods to promote the uptake of research findings into routine healthcare in clinical, organizational, or policy contexts.

Related Collections
With Collections, you can get published faster and increase your visibility.
Breaking Frameworks: Revisiting, Extending, Integrating, and Theorizing Implementation Frameworks
The field of implementation science has amassed a large number of frameworks3,4,5. These are sometimes also called models, but because the term “model” is used in many other contexts in research, we will use the term “framework.” While many of these frameworks express a goal of supporting research in the implementation of evidence-based practices and programs, researchers and especially new entrants to the field continue to express confusion and uncertainty about how to use existing frameworks and which to use for what purposes. New frameworks are often developed without clarity about how they fit within the existing corpus of frameworks.
Despite the large number of frameworks 4, their use often reflects a lack of deep understanding of the content of the frameworks. Implementation researchers often describe frustration with existing frameworks while continuing to use them. A major issue is that once published in a peer-reviewed venue, there is no clear path to suggest changes or updates to the frameworks. A few, such as the Consolidated Framework for Implementation Research (CFIR)6, the Exploration, Preparation, Implementation, Sustainment (EPIS) framework7,8, and the RE-AIM framework9, have been updated through processes determined by a relatively small group of researchers10; others remain essentially fixed as they were published, or updated once but not again11,12. This can lead to reification of the frameworks in their original form. These issues may constitute a major “sticking point” for advancing the science of implementation, as well as contributing to complexity for implementation practitioners who use frameworks as tools developed through the science. Emerging global health priorities, including health equity, structural racism, coloniality, climate and planetary health, digital transformation, and policy implementation, raise questions about whether existing frameworks adequately capture power, history, resource constraints, political economy, community agency, and cross-setting adaptation13. The increased geographic scope of published studies adds to concerns about whether theories and frameworks current in the literature support the broader scope.
We also note the importance of understanding the function of existing frameworks, most clearly addressed in the seminal 2015 paper by Nilsen describing an initial taxonomy of theories, models, and frameworks in implementation science5. We note that this paper is now over a decade old. Proposing additional taxonomic categories of frameworks, models, and theories is an important step yet to be taken.
This background informs this collection proposal. We are calling for manuscripts to address the issues, which may include methods (what methods can be used to update or extend existing frameworks), perspective or commentary manuscripts (why is this important), and empirical papers offering new insights, updates, and extensions of existing frameworks. We would also welcome papers that explicitly focus on theorizing based on existing frameworks, focusing on prediction and explanation rather than description14. However, manuscripts proposing new frameworks will be considered only if they clearly demonstrate how the proposed contribution builds on, revises, synthesizes, tests, or challenges existing frameworks, and why a new framework or a substantial extension is necessary. The existing body of frameworks and models within implementation science and practice constitutes an important catalog of knowledge. Our goal is to build on that existing knowledge.
Examples of topics include, but are not limited to:
- Innovative papers that develop new substantive theories or significant theoretical extensions to existing theories
- Methods for classifying and categorizing existing frameworks
- Proposing new domains and constructs for existing determinant frameworks
- Synthesizing across existing process frameworks to describe common elements and areas of departure
- Practical guidance on how to use existing tools such as the “Assess the Dissemination and Implementation Models Webtool” or useful new tools and approaches to help people select and use existing frameworks (these are likely to be assessed for Implementation Science Communications rather than Implementation Science)
This Collection welcomes submissions of a range of article types. Should you wish to submit to this Collection, please read the submission guidelines of the journal you are submitting to, i.e., Implementation Science or Implementation Science Communications, to confirm that the type is accepted by the journal you are submitting to.
Articles for this Collection should be submitted via our submission systems in Implementation Science or Implementation Science Communications. During the submission process, you will be asked whether you are submitting to a Collection. Please select "Breaking Frameworks: Revisiting, Extending, Integrating, and Theorizing Implementation Frameworks" from the dropdown menu.
Articles will undergo the standard peer review process of the journal in which they are considered, Implementation Science or Implementation Science Communications, and are subject to all of the journal’s standard policies. Articles will be added to the Collection as they are published.
The Editors have no competing interests with the submissions that they handle through the peer-review process. The peer review of any submissions for which the Editors have competing interests is handled by another Editorial Board Member who has no competing interests.
Publishing Model: Open Access
Deadline: Mar 09, 2027
Learning From the Past and Shaping the Future
Implementation Science has published 2,197 papers since its inception in 2006 (as of May 27, 2026). Implementation Science Communications has published 938 papers since it began in 2019 (also as of May 27, 2026). In addition to papers published in these two journals, a larger number of papers focusing on implementation science in health care have been published in other journals over the last 20 years, conservatively around 22,300. This is based on a PubMed search using a specific search string[1], conducted on May 27, 2026. It is important to note that landmark papers in the field were published before 2006. Our purpose in marking this anniversary is to reflect on the field as a whole.
While much of the growth in the literature has come from high-income countries, there has been an increase in the number and scope of papers from lower and middle-income countries, fueling the overall growth.
Arguably, the growth in the literature and underlying research studies shows that the science and practice of implementation have moved from the periphery to mainstream health research. We are interested in papers that document and analyze the change over the last couple of decades—although the history of the field prior to 2006 is also of interest—and propose how this shapes the future of the field. This may be based on bibliographic or citation analysis, surveys among researchers, or other sources. Papers that only review the past, without analysis and future direction, will not be seen as responding to this call.
Examples of topics include, but are not limited to:
- Content analysis or systematic reviews of empirical publications from Implementation Science and/or Implementation Science Communications
- Content analysis of editorials and research agenda-setting articles from both journals, including papers focusing on implementation science published in other journals
- Bibliographic/citation analysis of publications over the 20 years of IS, including other papers published in other journals
- Analyses of geographic, disciplinary, authorship, funding, or institutional patterns in implementation science
Submissions should include critical interpretive analysis of existing literature and provide new insights, ideas, and thoughts from reflection on the existing literature.
This Collection welcomes submissions of a range of article types. Should you wish to submit to this Collection, please read the submission guidelines of the journal you are submitting to, i.e., Implementation Science or Implementation Science Communications, to confirm that the type is accepted by the journal you are submitting to.
Articles for this Collection should be submitted via our submission systems in Implementation Science or Implementation Science Communications. During the submission process, you will be asked whether you are submitting to a Collection. Please select "Learning From the Past and Shaping the Future" from the dropdown menu.
Articles will undergo the standard peer-review process of the journal in which they are considered, Implementation Science or Implementation Science Communications, and are subject to all of the journal’s standard policies. Articles will be added to the Collection as they are published.
The Editors have no competing interests with the submissions that they handle through the peer-review process. The peer review of any submissions for which the Editors have competing interests is handled by another Editorial Board Member who has no competing interests.
[1] ("Implementation Science"[Mesh] OR "implementation science"[tiab] OR "implementation research"[tiab] OR "dissemination and implementation"[tiab] OR "translation science"[tiab] OR "knowledge translation"[tiab]) AND 2006:2026[dp]
Publishing Model: Open Access
Deadline: Mar 09, 2027
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in