Symptoms and respiratory infections: Insights from the UK 2022/2023 winter season
Published in Public Health and Statistics

Ever wondered about the likelihood of having the flu if you’ve got a fever? Or how your age influences the symptoms you experience if ill with RSV? And can we distinguish SARS-CoV-2 from other respiratory infections based on which symptoms people report? These are some of the questions our recent research study explored. In this blog post, I’ll explain the motivation behind our study and highlight our key findings.
What was our study about?
Respiratory infections affect lots of people every winter, and cause symptoms such as sneezing or fever. Often, these symptoms are mild, but such infections can also lead to more serious illness. Understanding how many people are getting different respiratory infections over time, and what symptoms they experience, is important to accurate diagnosis and effective treatment in the NHS. Getting more knowledge about these infections can also aid healthcare preparedness and inform vaccination policies.
Influenza A/B (flu) and respiratory syncytial virus (RSV) are two common causes of respiratory infection. Since the start of the COVID-19 pandemic, SARS-CoV-2 has also been co-circulating with these viruses. Our recent study investigated these three respiratory infections in the UK during the 2022-2023 winter season, along with self-reported symptoms. This study was based on a large household survey, the Office of National Statistics COVID-19 Infection Survey. Around 750 participants in the survey were randomly selected each week to have their nose and throat swabs PCR-tested for flu, RSV, and SARS-CoV-2. Our research study analysed this data using a range of statistical methods, including generalised additive models, which is a type of regression model.
What were the main findings?
Our study found that differentiating between flu, RSV, and SARS-CoV-2 based on symptoms alone may prove difficult. Symptom profiles were largely similar across the three viruses, with middle-aged participants being more likely to report symptoms than other age groups. Cough, sore throat, sneezing, and fatigue were amongst the most common symptoms for all three infections.
We did however see some differences between the three infections. For instance, RSV-positive people in our study generally reported fewer symptoms than those who tested positive for SARS-CoV-2 or the flu. In particular, fever was relatively uncommon amongst those with RSV. Importantly, we also observed considerable background rates of several symptoms, especially cough in young children, and fatigue and headache in middle-aged participants.
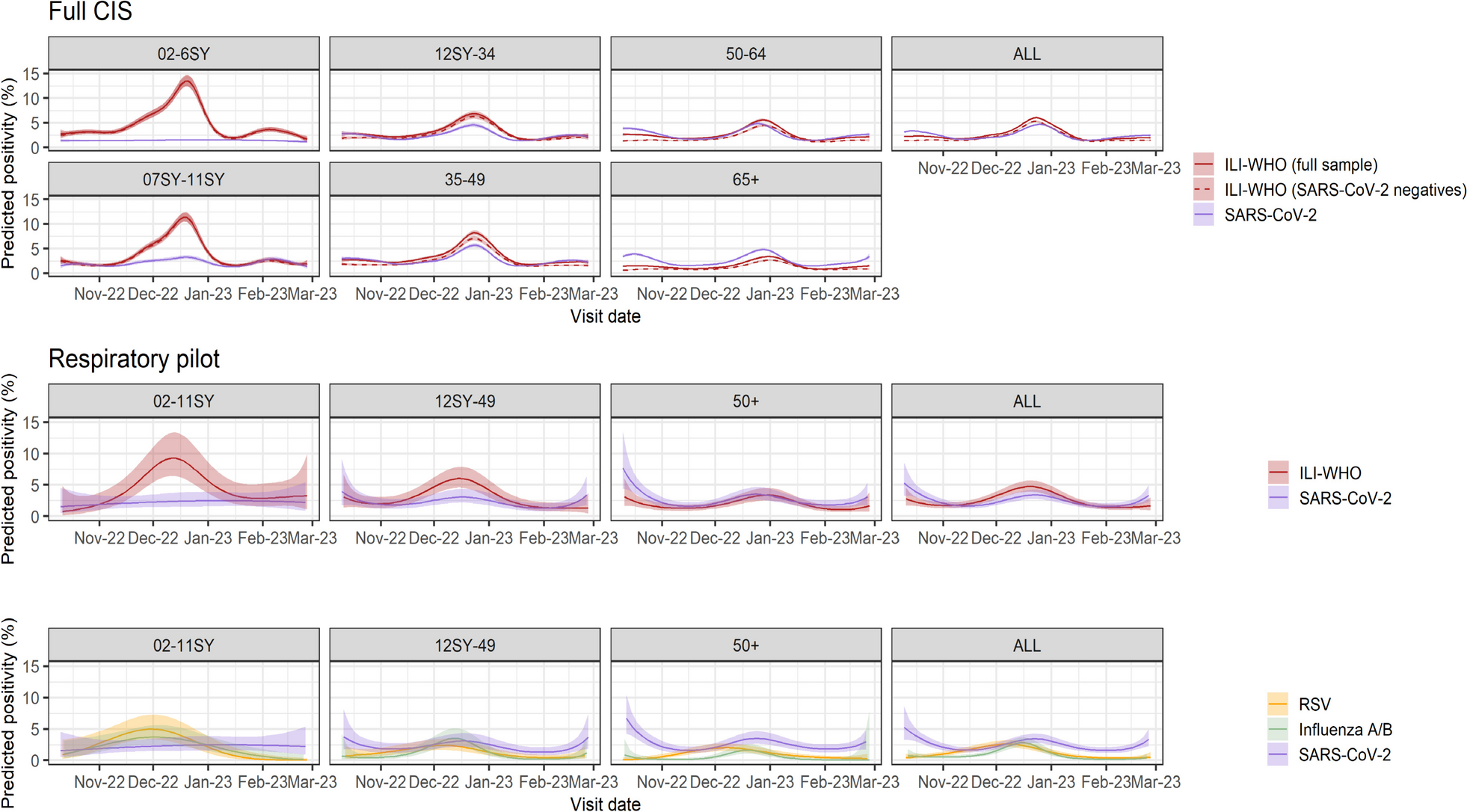
SARS-CoV-2 positivity was notably higher in adults than children, and RSV was more common in children below school year 12 than in older participants. Flu was also less common in participants aged 50 years and above than in younger age groups. By estimating incidence over time using a technique called Richardson-Lucy deconvolution, we found that flu peaks occurred earlier in children than older adults, with a delay of around 2 weeks.
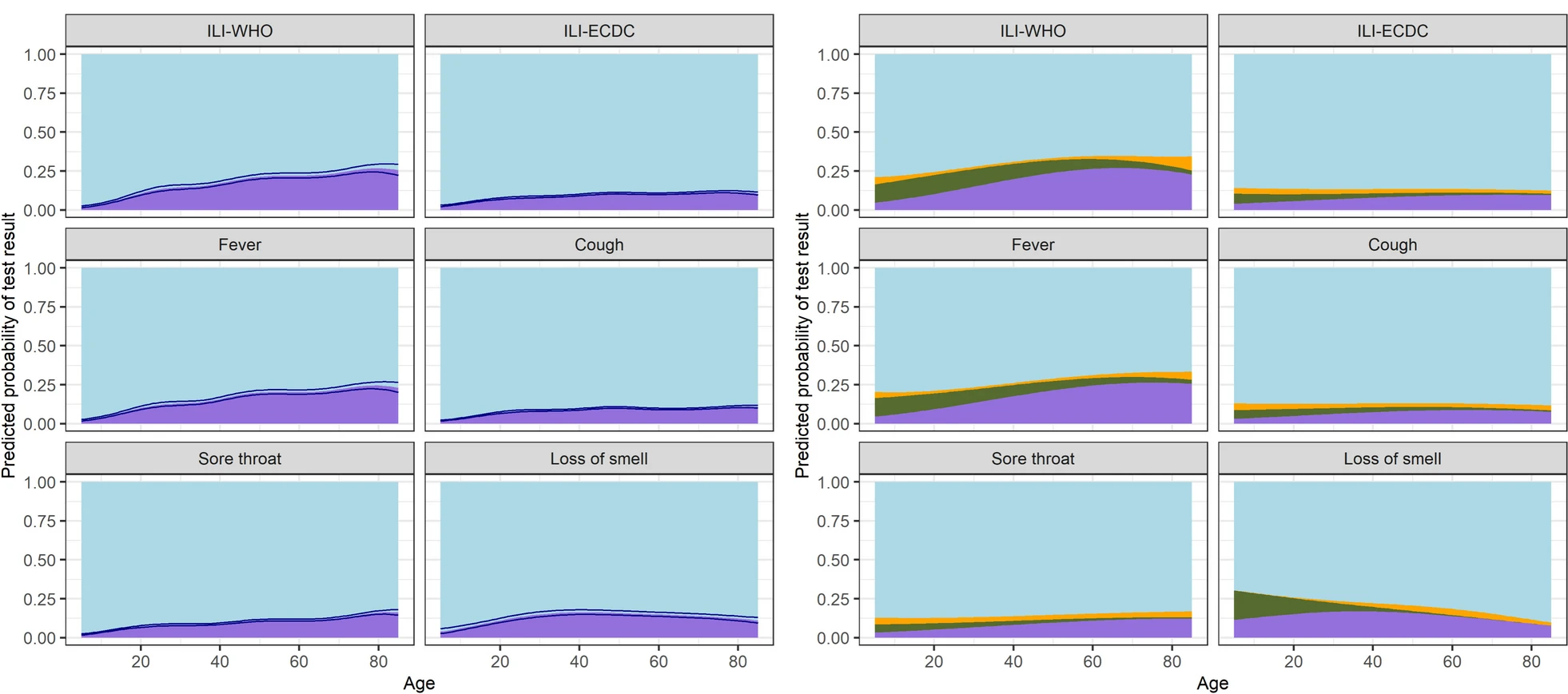
Many of the symptoms reported by people in the survey could not be explained by either of the three viruses we studied, highlighting the role of other infections such as the common cold. Fever was the symptom with the highest percentage of test-positive participants. The likelihood of testing positive for either of the three viruses generally increased by age across symptoms. However, even in older individuals reporting influenza-like-illness as defined by the WHO, only around ~30% had a positive test result for either SARS-CoV-2, the flu, or RSV. We also found that reporting flu vaccination in the past two winter seasons was associated with a lower likelihood of testing positive for flu in the current season.
What are the implications?
Given our findings, further research is needed on the role of other infections such as rhinovirus in causing respiratory symptoms. Future studies would benefit from having more specific data about the onset timing of symptoms and infections. However, our study emphasises the value of community-level data to understanding trends in respiratory infections and symptoms in people outside healthcare settings. Our study also raises important questions about the role of age in infection susceptibility, illness natural history, symptom reporting behaviour, and vulnerability to other symptom-inducing conditions. These questions provide promising avenues for future research, and highlight important considerations to the NHS and public health more broadly.
Follow the Topic
-
BMC Medicine
This journal publishes outstanding and influential research in all areas of clinical practice, translational medicine, medical and health advances, public health, global health, policy, and general topics of interest to the biomedical and sociomedical professional communities.

Related Collections
With Collections, you can get published faster and increase your visibility.
Advancing research and management of menopause
BMC Medicine is calling for submissions to our new Collection, Advancing research and management of menopause, focusing on new perspectives and care practices that support individuals during this significant life transition. This Collection seeks to advance the understanding and management of menopause by gathering clinical research on its physiological, psychological, and social dimensions. We welcome submissions that explore topics such as perimenopause, menopausal symptoms, early menopause, and menopausal hormone therapy (MHT) but also innovative interventions that help individuals navigate menopause beyond pharmacological treatment.
The menopause journey, encompassing the climacterium and the natural conclusion of reproductive years, is a pivotal phase in the lifecycle that impacts health and well-being. This Collection aims to consolidate research that addresses the multifaceted aspects of menopause, including its physiological, psychological, and social dimensions, thereby offering a comprehensive view of the experiences faced during this transition.
Advancements in the understanding and management of menopause have opened new avenues for improving health. Research indicates that the heterogeneity of menopause (surgical, spontaneous, induced, early) as well as the heterogeneity of MHT (formulations, duration, age of initiation relative to menopause onset, cyclicity, progestrogen/progestin) can differentially affect outcomes, yet are not as well understood or studied. Studies on menopausal symptoms have enhanced our understanding of their prevalence and impact on daily life. Research on menopausal hormone therapy has evolved, shedding light on its benefits and risks, while growing evidence highlights a number of other effective options for managing common menopausal symptoms. Additionally, the focus on long-term effects of menopause, e.g. osteoporosis and prevention strategies, underscores the necessity for ongoing research and tailored interventions during and after this transition.
Continued exploration in this field promises to yield significant insights, potentially leading to the development of novel therapeutic options, personalized management strategies, and a broader understanding of the heterogeneity of menopause and individuals’ experiences. As research progresses, we may see improved guidelines for addressing early menopause and premature ovarian insufficiency, ultimately empowering individuals to navigate this life stage with confidence and health.
Topics of interest include but are not limited to:
- Management strategies for menopausal symptoms
- MHT: risks and benefits
- Post-menopausal osteoporosis prevention
- Ovarian aging and its implications
- Understanding early menopause and premature ovarian insufficiency
This collection supports and amplifies research related to SDG 3: Good Health & Well-Being and SDG 5: Gender Equality.
Publishing Model: Open Access
Deadline: Oct 17, 2026
Cardiac immunity and inflammation
BMC Medicine invites submissions to a new Collection focused on the interplay between cardiac immunity and inflammation. We welcome original research, translational studies, and comprehensive reviews that elucidate the underlying mechanisms, clinical consequences, and therapeutic opportunities arising from immune-cardiac interactions. By highlighting the importance of this link, we aim to foster collaboration and advance our understanding of how to improve patient outcomes in heart disease.
The intersection of immunity and cardiovascular biology represents a transformative frontier in modern medicine. Recent studies have highlighted the role of immune responses in various heart conditions, including myocarditis, cardiac xenotransplantation, and heart failure. Inflammation is increasingly recognized as a contributing factor to the pathogenesis and residual risk factor of cardiovascular diseases. This Collection aims to explore the mechanisms by which immune responses influence cardiac function, the role of clonal hematopoiesis and heart disease, and the implications of such interactions for cardiac outcomes.
Understanding cardiac immunity and inflammation is crucial for developing more targeted therapies and accurate CVD risk prediction. Past advances provided insights into the inflammatory processes involving cardiovascular conditions, leading to innovative approaches for diagnosis and treatment. For instance, the identification of biomarkers such as C-reactive protein enhances our ability to assess inflammation in patients with cardiovascular disease. Furthermore, the intersection of cardio-oncology has opened new avenues for research into how cancer therapies influence cardiac immune responses, emphasizing the need for a multidisciplinary approach to patient management.
Continued research in this field holds promise for unveiling drug discovery targets and strategies to mitigate inflammation-related cardiac damage. As we deepen our understanding of the immune mechanisms at play, we may see the development of more clinically relevant models of human disease and precision medicine approaches tailored to individual patients. The integration of this knowledge with advancements in technology, such as biomarker discovery and imaging techniques, could revolutionize the way we approach cardiac care.
Topics of interest include (but are not limited to):
- Role of immunity in cardiovascular biomedicine
- Systemic and cardiac-specific inflammatory pathways
- Residual inflammatory risk, e.g. “SMuRF-less but inflamed”
- Cross-organ communication and immune crosstalk
- Structural and functional cardiac remodeling driven by inflammation
- Novel biomarkers and prediction models
- Clonal hematopoiesis
- Cardio-oncology & therapy-induced immune modulation
- The role of immunity in cardiac xenotransplantation including partial heart transplantation
- Exposome/environmental exposures
- Epigenetic regulation of cardiac immunity and inflammation
- Immune memory and trained immunity in cardiovascular contexts
- Multi-omics integration (epigenomics, transcriptomics, proteomics) in cardiac disease
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
This Collection supports and amplifies research related to SDG 3 (Good Health and Well Being).
Publishing Model: Open Access
Deadline: Feb 01, 2027


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in