Sex-specific lipidome changes associated with diabetes
Published in Cell & Molecular Biology and General & Internal Medicine


The research involved 360 participants: 91 with T1D, 91 with T2D, 74 prediabetic individuals, and 104 controls. All participants were free from previous cardiovascular or chronic kidney disease. The study utilized untargeted lipidomic analysis through Ultra-high performance liquid chromatography-electrospray ionization mass spectrometry (UHPLC-ESI-MS) to assess lipid profiles. Multiple linear regression models were employed to examine the associations of different lipid classes with diabetes, while considering both sex-specific differences and glycemic states.
Study findings
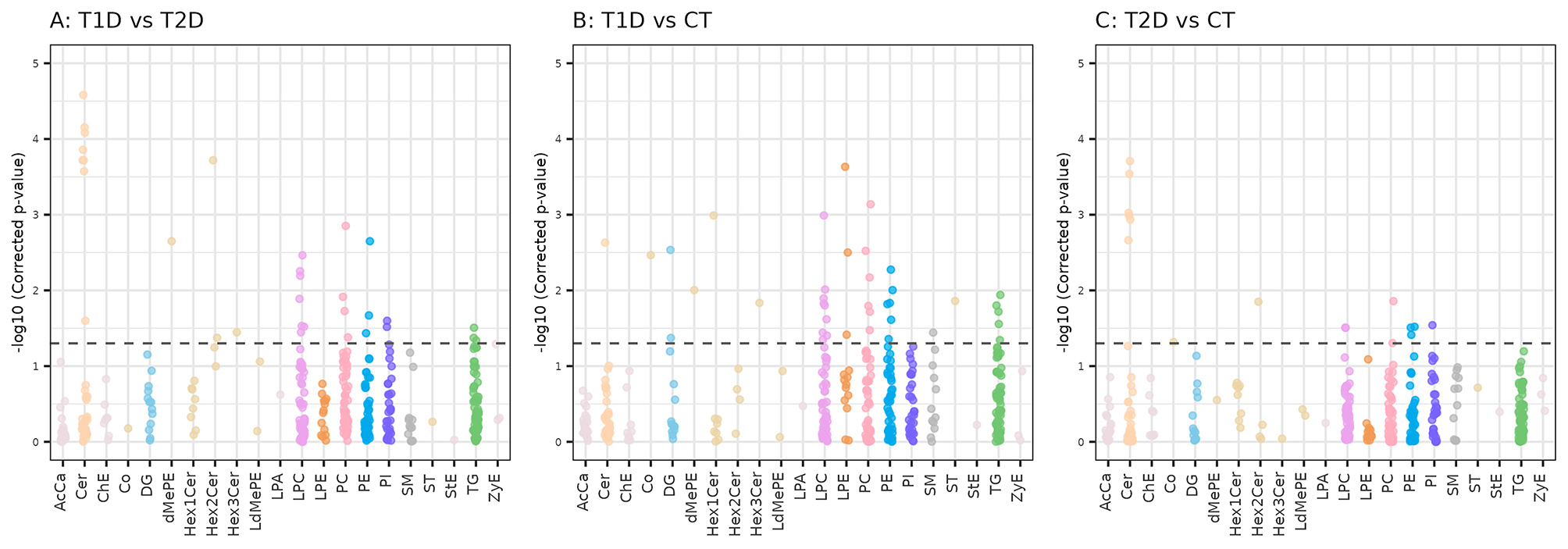
The study identified 54 unique lipid subspecies from 15 unique lipid classes, highlighting a diverse lipidomic profile associated with diabetes.
Lysophosphatidylcholines (LPC) and ceramides showed opposite effects in subjects with T1D and subjects with T2D. Lysophosphatidylcholines were significantly up-regulated in T1D participants but down-regulated in those with T2D. This suggests that LPC metabolism differs markedly between these two types of diabetes. This increase in LPC levels may correlate with increased LCAT activity, which is involved in lipid metabolism, particularly the synthesis of phosphocholine and cholesteryl esters from LPCs and phosphatidylcholine.
Ceramides displayed the opposite trend compared to LPCs; they were found to be up-regulated in subjects with T2D while showing down-regulation in T1D. Variants such as 1-deoxyceramides exhibited a significant increase in T2D, marking them as important indicators of the disease. These findings indicate a clear alteration in ceramide metabolism in type 2 diabetes that may influence insulin signaling pathways, potentially worsening insulin resistance.
Phosphatidylcholines (PC) were predominantly down-regulated in the subjects with type 1 diabetes; this may have implications for membrane integrity and function. This down-regulation contributes to the overall altered lipid profile observed in T1D.
Interestingly, the study identified sex-specific lipidomic differences. For instance, lipid alterations were notably more pronounced in men regarding certain ceramides. Specifically, specific ceramide molecules were significantly decreased only in men with T1D. Additionally, higher levels of phosphatidylcholines were present in normoglycemic women than in men. These findings point to the role of hormonal factors in determining sex-specific lipid metabolism differences.
We also analyzed possible associations of lipid classes with the glycemic state, i.e. normoglycemia, prediabetes and type 2 diabetes. A gradual increase in 1-deoxyceramides was seen progressing from normoglycemia through prediabetes to T2D, indicating these lipid species might serve as potential early biomarkers for diabetes progression.
Clinical and research implications
The findings underscore a substantial disruption in lipid metabolism for both types of diabetes, indicating that further investigation into lipidomic profiles may yield critical insights into diabetes pathophysiology. This could lead to enhanced understanding of the disease mechanisms and the identification of novel biomarkers for diabetes. Furthermore, from the clinical point of view, our results suggest the need for sex-specific strategies in diabetes management. This personalized approach to treatment could enhance patient outcomes and open avenues for tailored therapeutic interventions. Moreover, the future potential introduction of lipidomic profiling characterization into routine clinical assessments could contribute to more precise management of diabetes and its complications.
Overall, this study contributes relevant knowledge to the field of diabetes research, emphasizing the potential of lipidomics in personalizing treatment strategies while highlighting the importance of sex differences in metabolic responses.
Follow the Topic
-
Cardiovascular Diabetology
This journal considers manuscripts on all aspects of the diabetes/cardiovascular interrelationship and the metabolic syndrome; this includes clinical, genetic, experimental, pharmacological, epidemiological and molecular biology research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Incretin-Based Therapies in Type 2 Diabetes and Obesity: Current Evidence and the Evolving Cardiometabolic Landscape
Cardiovascular Diabetology features a Collection on "Incretin-Based Therapies in Type 2 Diabetes and Obesity: Current Evidence and the Evolving Cardiometabolic Landscape". This is a companion Collection with Cardiovascular Diabetology - Endocrinology Reports with the title "Pleiotropic Actions of Incretin-Based Therapies".
Building upon the growing recognition of cardiometabolic organ protection as a central therapeutic goal, incretin-based therapies have reshaped the management of type 2 diabetes and obesity, extending their clinical relevance far beyond glycemic control. Large-scale cardiovascular outcome trials (CVOTs) have shown that glucagon-like peptide-1 receptor agonists (GLP-1RAs) significantly reduce major adverse cardiovascular events (MACE), redefining cardiometabolic risk management and influencing contemporary therapeutic strategies. Targeting the glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) pathways, these agents enhance glucose-dependent insulin secretion, promote weight reduction, and exert multi-organ effects. Growing evidence supports their impact on vascular function, myocardial metabolism, renal protection, metabolic dysfunction-associated steatotic liver disease (MASLD), and systemic inflammation.
Three principal pharmacological approaches currently characterize incretin-based therapy:
- GLP-1 receptor agonists (GLP-1RAs), mostly injectable medications with proven improved cardiovascular outcomes and weight-reduction.
- Dual GIP/GLP-1 receptor agonists, newer solely injectable medications designed to enhance glycemic control and weight-reduction efficacy.
- DPP-4 inhibitors (also known as gliptins), oral medications which modestly increase endogenous incretin levels and have no impact on cardiovascular outcomes or body weight.
Beyond glucose lowering, incretin-based therapies are increasingly positioned within the broader cardiometabolic framework, with emerging data supporting cardiovascular and renal protection, as well as effects on endothelial function, atherosclerosis, heart failure phenotypes, and chronic kidney disease progression.
Areas of interest include, but are not limited to:
- Classic antidiabetic, anti-obesity and cardioprotective effects
- Cardiovascular outcomes and mechanistic correlates
- Endothelial and vascular biology
- Myocardial metabolism and heart failure subtypes
- Novel renal and hepatoprotective actions
- Optimization and individualized use of existing GLP-1 receptor agonists
- Development of novel GLP-1 receptor agonists and multi-agonist (dual and triple) strategies
- Emerging extra-metabolic actions, including anti-inflammatory and neuroprotective effects
- Combination therapies, including co-formulations with insulin or SGLT2 inhibitors
- Innovative delivery systems, including non-injectable and implantable approaches
- Real-world comparative effectiveness, long-term safety, adherence and treatment durability
This Collection welcomes original research, translational studies, and comprehensive reviews and meta-analyses that provide novel mechanistic insight or clinically relevant evidence to advance understanding of the expanding role of incretin-based therapies in cardiometabolic medicine.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the journal editorial board. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com.
Publishing Model: Open Access
Deadline: Dec 13, 2026
Cardiovascular-Kidney-Metabolic (CKM) Syndrome: Risk Stratification, Prognostic Implications and Therapeutic Innovation
Cardiovascular Diabetology features a Collection on "Cardiovascular-Kidney-Metabolic (CKM) Syndrome: Risk Stratification, Prognostic Implications and Therapeutic Innovation". This is a companion Collection with Cardiovascular Diabetology - Endocrinology Reports with the title "Endocrine Drivers and Clinical Implications of the Cardiovascular–Kidney–Metabolic Syndrome" and with BMC Cardiovascular Disorders with the title "Cardiovascular-Kidney-Metabolic (CKM) Syndrome: diagnosis and management of a systemic disorder".
The cardiovascular–kidney–metabolic (CKM) syndrome describes the multidirectional interactions linking excess adiposity, metabolic dysfunction — particularly insulin resistance and type 2 diabetes — chronic kidney disease, and cardiovascular involvement. In affected individuals, metabolic abnormalities frequently coexist with subclinical or overt cardiovascular disease.
Rather than representing a simple clustering of comorbidities, CKM represents a pathophysiological continuum in which metabolic dysregulation drives progressive cardiovascular and renal injury through inflammation, oxidative stress, renin–angiotensin–aldosterone system activation, lipotoxicity, and endothelial dysfunction, ultimately promoting adverse cardiac remodeling, heart failure, and cardiorenal syndrome.
The American Heart Association has proposed a staged framework ranging from individuals without metabolic risk (stage 0) to isolated adiposity (stage 1), metabolic or kidney disease without overt cardiovascular involvement (stage 2), subclinical cardiovascular disease (stage 3), and symptomatic cardiovascular disease (stage 4). This framework aims to facilitate earlier risk identification and integrated cardiovascular prevention across the CKM spectrum.
Areas of interest include, but are not limited to:
- Early detection of multiorgan abnormalities across CKM stages
- Diagnostic laboratory and imaging biomarkers
- Digital health tools for remote monitoring of blood pressure, weight, glycemia, and kidney function
- Application of explainable artificial intelligence (XAI) for risk prediction and treatment selection
- Geographical epidemiology of CKM syndrome
- Social determinants contributing to CKM development and progression
- Life-course determinants, including childhood obesity and gestational diabetes
- Multi-target non-pharmacological interventions
- Established pharmacological therapies (e.g., SGLT2 inhibitors, GLP-1 receptor agonists, non-steroidal mineralocorticoid receptor antagonists)
- Emerging therapies, including RNA-based approaches, incretin combinations, and anti-inflammatory strategies
This Collection invites original research, systematic reviews, and meta-analyses that contribute to improved risk stratification, prognostic assessment, and therapeutic innovation within the integrated CKM framework.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this Collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the journal editorial board. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com.
Publishing Model: Open Access
Deadline: Nov 23, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in