Spatial and Contextual Disparities of Influential Factors of Adult Obesity among Communities in Chicago
Published in Social Sciences, Earth & Environment, and Ecology & Evolution
This study examines the nineteen demographic, socioeconomic, behavioral, and environmental factors influencing adult obesity across Chicago’s 77 community neighborhoods. Using advanced geographic methods—including geo-visualization, Exploratory Spatial Data Analysis (ESDA), Analysis of Variance (ANOVA), and Geographically Weighted Regression (GWR), the study provides a nuanced understanding of how obesity patterns cluster geographically and how multifaceted risk factors vary spatially across the city.
Data & Methods
The demographic data (percentage of White, African American, Hispanic, and other minority groups) from the American Community Survey (ACS). Adult obesity data came from the Chicago Health Atlas. Physical environment determinants included Sidewalk Quality, Land Use Mix Index (LUMI), Number of Parks, Walkability Index (WI), Social Vulnerability Index (SVI), and density of Fitness Centers. Behavioral data, such as adult smoking, psychological distress, neighborhood safety, and loneliness, as well as socioeconomic variables, including the Hardship Index (HI), unemployment rate, Economic Diversity Index (EDI), poverty, food insecurity, and public assistance income, were also obtained from the Chicago Health Atlas. Together, these variables illustrate a complex interplay of contextual factors determining health outcomes. The analytical framework involved spatial statistics to measure clustering and spatial relationships. Local Moran’s I identified obesity "hotspots" and "coldspots," showing statistically significant geographic controls. GWR allowed coefficients to vary spatially, rather than assuming uniform effects across the city, providing a local rather than a global view of the factors driving obesity.
Spatial Distribution of Adult Obesity
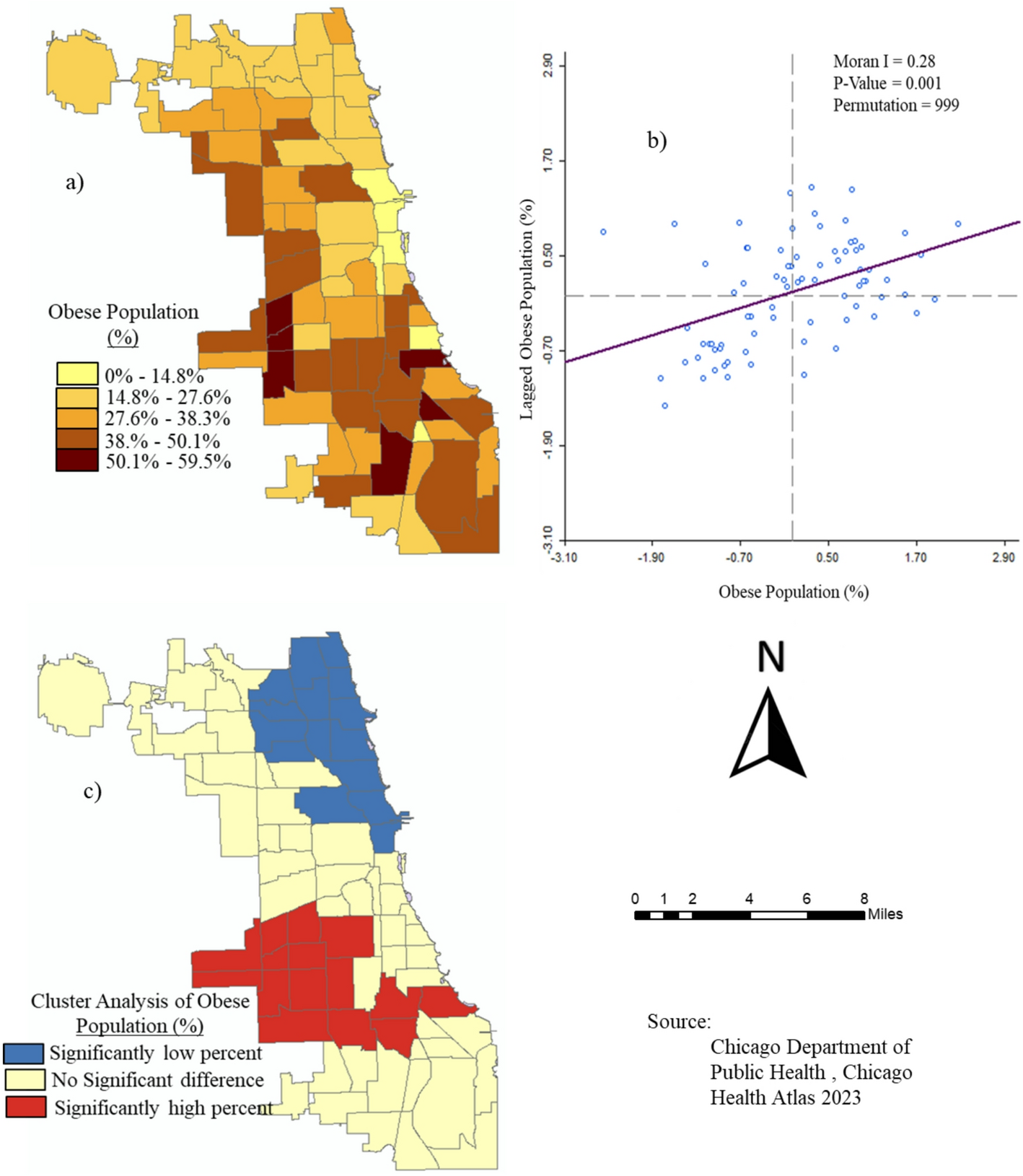
The spatial analysis revealed substantial variation at the neighborhood level. Obesity rates ranged from under 10% in parts of the Near South Side to nearly 60% in places such as Archer Heights. Chicago’s average obesity prevalence (32%) is comparable to the Illinois average but lower than the U.S. average, yet it far exceeds the global average. ANOVA confirmed statistically significant differences across Healthy Chicago Equity Zones (HCEZs), with Central, North, and Far North zones showing significantly lower rates, while Southwest and West zones exhibited the highest burdens. Moran’s, I detected significant positive spatial autocorrelation (I = 0.28), confirming obesity clustering rather than random distribution. Southwestern and western neighborhoods formed consistent high-obesity clusters; northern and central zones formed low-obesity clusters.

Fig. 1 Spatial analysis of the pattern of the adult obese population rate among Chicago neighborhoods: a) adult obese percentage, b) Global Spatial autocorrelation for geographic control, and c) cluster analysis
Disparities in Adult Obesity Determinants in space and context
Race and ethnicity emerged as powerful predictors of spatial location, with the White residents having a strong negative association with obesity rates (R² = 0.39), while minority residents showed strong positive associations (R² = 0.39). The strongest associations among minorities occurred in historically Black neighborhoods on the West and South Sides. Roughly 32% of neighborhoods had little to no association with demographic obesity, particularly in more racially mixed northern communities. On the other hand, Environmental determinants such as sidewalk quality, land use mix, park distribution, walkability, and fitness center density. Among environmental variables, walkability showed the strongest relationship (R² = 0.43), followed by sidewalk quality (R² = 0.33) and fitness centers (R² = 0.23). Surprisingly, the number of parks and the land use mix showed weak associations (R² = 0.06–0.08), suggesting that the mere presence of parks does not guarantee usage, accessibility, or quality, especially in neighborhoods that are not safe for walking and other physical activities.
Table 1: Spatial Relationships of Percentages of Adult Obesity and Demographic Composition of Chicago Neighborhood Communities

Similarly, Behavioral factors like Adult smoking and psychological distress were positively associated with obesity, while neighborhood safety was negatively associated. The findings support broader literature linking obesity to chronic stress, trauma, social isolation, and unsafe environments that limit outdoor physical activity. Lastly, the socioeconomic stressors showed some of the strongest and most statistically significant associations with obesity. Hardship Index and unemployment rate each explained 35% of the variance in obesity rates, while food insecurity, poverty, EDI, and public assistance income also showed moderate associations. Over half of the neighborhoods, however, showed no association, indicating that socioeconomic determinants alone cannot explain all variation, which underscores the multifactorial nature of obesity.
Conclusion
Adult obesity in Chicago communities is shaped by a complex interplay of demographic, environmental, behavioral, and socioeconomic factors operating within spatially distinct contexts. Obesity does not occur randomly; it clusters in neighborhoods characterized by racial segregation, economic hardship, lower walkability, limited fitness infrastructure, higher smoking rates, and psychological distress. Therefore, effective interventions must consider spatial heterogeneity and tailor strategies to local conditions. Policies should target structural inequities, enhance physical environments, increase access to health-promoting resources, and address behavioral health needs. Despite limitations including autocorrelation biases and multicollinearity, the study provides a robust empirical foundation for spatially informed public health planning and equity-focused interventions in Chicago.
Follow the Topic
-
Discover Public Health
This is an open access journal publishing research from all fields relevant to public health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Promoting Healthy Diets and Food Security across Global Public Health Systems
The interconnection between healthy diets and food security is a critical concern for global public health systems, particularly in the context of escalating population growth, climate change, and socioeconomic disparities. Proper nutrition is essential for overall health and well-being; however, millions worldwide face malnutrition in its various forms, including undernutrition, micronutrient deficiencies, and obesity. Food security encompasses not only the availability of food but also its accessibility, utilization, and stability. Addressing these complex challenges is vital for achieving sustainable development goals and improving health outcomes across diverse populations.
This Collection is motivated by the urgent need to strengthen the integration of health policy with healthy diet promotion and food security within public health frameworks. As nations work to build resilient health systems, innovative strategies that promote healthy eating and ensure food security are essential. This Collection aims to gather interdisciplinary insights and research that address these pressing issues, fostering collaboration among public health experts, nutritionists, policymakers, and community stakeholders.
The purpose of this Collection is to provide a platform for sharing research findings and practical solutions that enhance healthy diets and food security through effective health policies. We welcome contributions that explore policy interventions, community-based initiatives, and innovative programs focused on promoting nutrition education and improving food access. By highlighting diverse perspectives and successful models, this Collection seeks to inform future public health strategies and contribute to the development of effective, equitable food systems worldwide.
Topics of interest include, but are not limited to:
- Evidence-based community interventions to enhance food security
- The influence of health policy on food systems and public health outcomes
- Global case studies demonstrating effective food access and health promotion
This Collection supports and amplifies research related to SDG 2 and SDG 3.
Keywords: healthy diets; food security; nutrition promotion; malnutrition; public health; health policy; food access and availability
Publishing Model: Open Access
Deadline: Dec 05, 2026
The Economics of Longevity: Health Expenditure and Societal Implications for Public Health Systems
The relationship between health investment and life expectancy has long been a focal point in public health research and policy. As nations grapple with rising healthcare costs and varying health outcomes, understanding how financial allocations influence population health becomes increasingly critical. Numerous studies have illustrated that increased spending on health services often correlates with improvements in life expectancy; however, the complexities of this relationship are not fully understood. Factors such as socioeconomic status, healthcare accessibility, and the efficiency of health systems play significant roles in determining how investments translate into health outcomes.
At the national level, health investments primarily encompass government expenditure on healthcare systems, public health initiatives, and health infrastructure. Nations that allocate substantial resources toward healthcare often experience better health outcomes and increased life expectancy among their populations. For instance, countries with robust healthcare funding tend to provide more comprehensive services, including preventive care, chronic disease management, and health promotion programs, all of which contribute to enhanced population health. However, it is crucial to consider how these investments are distributed across different segments of the population. Inequities in health spending can exacerbate existing disparities, leading to significant differences in life expectancy among various demographic groups. Effective health investment strategies must address these disparities to ensure that improvements in life expectancy are equitable and inclusive.
The motivation for this Collection arises from the urgent need to bridge the gap between health expenditures and tangible improvements in life expectancy. Recent global health crises and ongoing disparities in health outcomes across different populations have underscored the necessity for a deeper exploration of how resource allocation affects health dynamics. This Collection seeks to provide a platform for researchers and practitioners to discuss empirical evidence, theoretical frameworks, and innovative approaches to understanding these critical interactions. By fostering dialogue around effective health investment strategies, we aim to contribute to the development of more equitable and efficient health systems worldwide.
The purpose of this Collection is to gather comprehensive research that elucidates the dynamics between health investment and life expectancy across diverse contexts. We welcome contributions that analyze historical trends, comparative studies, and policy evaluations, as well as those that explore the implications of financial investments on health equity. By highlighting interdisciplinary perspectives and fostering collaboration, this Collection aspires to advance the discourse on optimizing health investments for improved population health outcomes.
Topics of interest include, but are not limited to:
- Economic evaluations of health interventions
- Policy impacts on health spending and life expectancy
- Health equity and investment disparities
- Longitudinal studies on health expenditures and population health
This Collection supports and amplifies research related to SDG 3.
Keywords: health expenditure; healthcare economics; life expectancy; economic evaluation; population health; health investment; health policy
Publishing Model: Open Access
Deadline: Sep 04, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in