Tertiary lymphoid structures potentially promote immune checkpoint inhibitor response in SMARCB1-deficient medullary renal cell carcinoma
Published in Biomedical Research
How did this get started?
We were concerned by the introduction of a newly defined molecular category named SMARCB1-deficient medullary renal cell carcinoma (RCC). Renal medullary carcinoma (RMC), the primary type of SMARCB1-deficient medullary RCC, has shown responsiveness to platinum-based chemotherapy. Consequently, the NCCN Guidelines version 1.2025 recommend platinum-based chemotherapy as the preferred first-line therapy for RMC. However, given the lethal nature of SMARCB1-deficient medullary RCC, the survival benefit of chemotherapy remains limited, with significant side effects impacting patients' quality of life. This highlights the urgent need for more effective and less toxic therapeutic options. Previous studies have reported discouraging outcomes with tyrosine kinase inhibitor (TKI) or immune checkpoint inhibitor (ICI) monotherapy, showing a median treatment duration of less than 9 months. A study by Msaouel et al. revealed increased hypoxia-associated gene expression and high immune cell infiltration in RMC, providing a theoretical basis for combining TKI with ICI. Inspired by this study, we chose to use ICI combination therapy as the first-line treatment for this aggressive subtype.
What was the result?
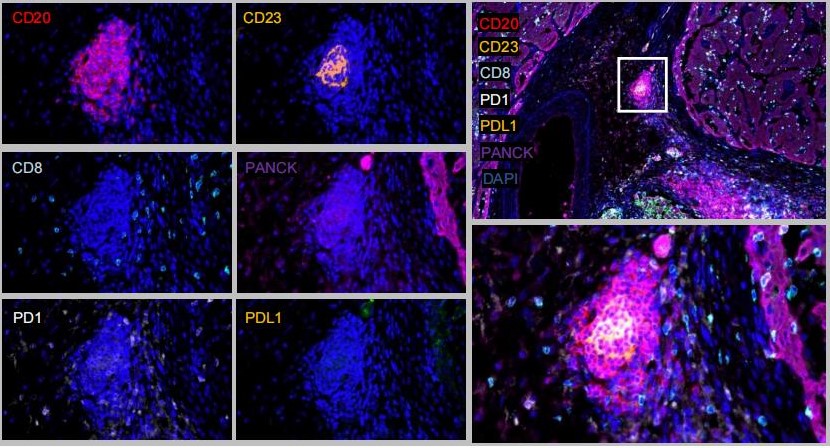
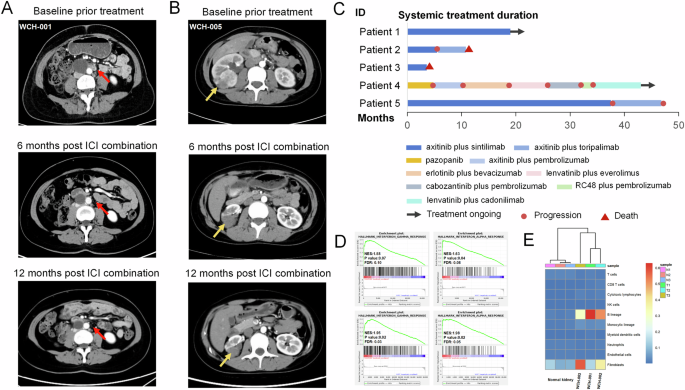
Outcomes exceeded our expectations. In the metastatic setting, four patients were administered a first-line regimen of TKI in combination with ICI with a mPFS of 12.3 months. This result from combination therapy is notably favorable compared to previous monotherapy studies. Nonetheless, heterogeneity in treatment response was observed, with two patients achieving partial responses. We sought to understand the underlying mechanism for this variation in efficacy. Meylan et al. identified a 29 genes signature included immunoglobulin genes, B cells markers, T cells markers, fibroblasts markers and complement protein coding genes, which reflects RCC with tertiary lymphoid structures (TLSs). We then analyzed the transcriptomic profile of RMC patients and found elevated TLS signature scores in tumor tissue compared to adjacent tissue. Previous studies have shown that intratumoral TLSs with mature germinal centers are associated with favorable responses to ICI treatment in several solid tumors. This led us to hypothesize that TLS formation might explain the response to immunotherapy in SMARCB1-deficient medullary RCC. To test this hypothesis, we performed morphological evaluations using H&E staining and multiple immunofluorescence. In the response group, CD20+ B cells aggregated with an enrichment of CD23+ germinal center cells in the central zone, while CD8+ T cells were observed adjacent to the B cell aggregation. In contrast, such mature secondary follicles were absent in the non-response group.
What still needs to be done?
A lot. A larger cohort is essential to further investigate responses to ICI combination therapy. Additionally, acquiring metastatic surgery or biopsy samples after treatment is part of our plan, which would facilitate the dynamic monitoring of TLS changes before and after immunotherapy.
You can read the paper at:
Tang, YF., Chen, JR., Zhang, MX. et al. Tertiary lymphoid structures potentially promote immune checkpoint inhibitor response in SMARCB1-deficient medullary renal cell carcinoma. NPJ Precis Oncol (2024).
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Demystifying Rare Breast Cancers
Publishing Model: Open Access
Deadline: Jul 16, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in