The need for predictive biomarkers of tumor hypoxia
Published in Cancer, Protocols & Methods, and Computational Sciences
Tumor hypoxia denotes regions within solid tumors where the oxygen partial pressure is approximately below 15 mmHg (equivalent to 2% oxygen in the gas-phase) [Singleton et al., 2021]. An exact threshold for tumor hypoxia is difficult to define, because oxygenation varies over time and between different tissues. A common characteristic of hypoxic cancer cells is that they exhibit a greater degree of resistance to radiation- and chemotherapy than their well-oxygenated counterparts [Janssen et al., 2005]. Consequently, hypoxia is known to contribute to treatment failure and thereby to cancer recurrence.
In our study, we investigated hypoxic regions of tumor tissue from head and neck squamous cell carcinoma (HNSCC) xenograft models. Considering that patients with locally advanced HNSCC still face a risk of disease recurrence of around 40% to 60% despite improvements in therapy [Machiels et al., 2020], hypoxia cannot be disregarded as contributing factor. Several studies demonstrated that the hypoxic volume of tumors inferred from positron emission tomography (PET) imaging is strongly associated with local-regional control and overall survival in HNSCC [Zschaeck et al., 2020].
What is currently missing in spite of extensive research are predictive molecular and clinically applicable biomarkers for hypoxia.
Predictive markers have the ability to estimate the likely outcome of a given therapy and thereby allowing the selection of the most promising treatment for an individual patient. Besides risk stratification, molecular biomarkers are crucial for identifying potential new targets. For HNSCC, many hypoxia gene expression signatures have been proposed with the aim of identifying patients at high-risk. Several of these gene signatures have shown promise in stratifying patients in earlier radiotherapy protocols [Toustrup et al., 2011; Eustace et al., 2013]. However, in recent randomized trials, these proposed gene signatures failed to stratify patients with locally advanced HNSCC by hypoxia to prognosticate loco-regional control [Grégoire et al., 2021; Thomson et al., 2023].
The reasons for this predictive shortcoming are likely to be manifold:
- Traditionally, gene signatures were often derived from cell lines exposed to hypoxic conditions or by a pre-selection of genes from hypoxia-associated pathways [Harris et al., 2015]. After an initial exploration phase, gene signatures are regularly refined to encompass a reduced set of candidates. Both, the exploration and subsequent selection process may oversimplify the phenomenon of hypoxia. While simplification promotes the translation into clinical practice, it may fail to capture the clinically relevant heterogeneity of hypoxia in patients.
- Since the development of the aforementioned hypoxia signatures, treatment regimens have evolved. Today, radiotherapy is carried out using intensity modulated radiation therapy, enabling inhomogeneous dose distribution and thus allowing a more targeted therapy than in previous times. In addition, radiotherapy is typically no longer applied alone but concomitantly with chemotherapy. Consequently, existing biomarkers may no longer reflect the molecular environment of surviving cancer cells.
- For similar reasons, it may be insufficient to evaluate hypoxia once before treatment. Instead, it may require to identify surrogates, which effectively monitor the degree of hypoxia over time. For PET imaging, it was shown that residual hypoxia during radiochemotherapy is strongly correlated with loco-regional control in patients with locally advanced HNSCC [Löck et al., 2017].
- Lastly, broader validations are needed to confirm the robustness of signatures before translating them into clinical applications. Apart from pre-clinical experiments, it is essential to assess data from diverse and multiple (ideally multi-center) patient cohorts retrospectively.
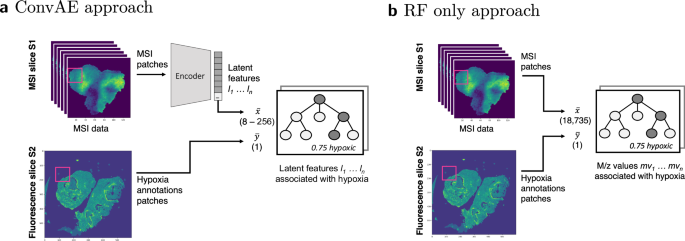
Drawing from these observations our manuscript [Bitto et al., 2024] was built; in 1), it is evident that new methodologies need to be explored to derive biomarkers. Spatial omics technologies bridge molecular and imaging modalities, offering a more nuanced understanding of the spatial heterogeneity of hypoxia. Accordingly, the effective processing of this data is key to derive credible molecular biomarkers. Our proposed workflow enables to investigate hypoxia on a broader scale by avoiding artificial elimination of potential candidates and correlating features.
To address the observations 2) and 3), we plan to evaluate also mass spectrometry imaging data from HNSCC xenografts subjected to a treatment protocol comparable to those in patients (e.g., fractionated radiochemotherapy). This enables a narrowing of peptide candidates based on their presence in residual and thus therapeutically significant hypoxia. To account for observation 4), we plan to verify the involvement of the identified proteins in hypoxia and radioresistance in vitro. Their relevance will then be evaluated retrospectively in different HNSCC patient cohorts.
While we highlighted in our paper [Bitto et al., 2024] how to retain low-abundant signals of hypoxia, this workflow builds a solid foundation to extract also other features that exhibit spatial variability. Among these features relevant in cancer are metastasis or cancer stem cells. However, feature extraction is not limited to a particular disease. Being technology-agnostic, our workflow also supports the analysis of other spatial omics data, like spatial transcriptomics. On a larger scale, our work contributes to broadening the scope of spatial omics research to low-abundant signals.
References
- Bitto V, Hönscheid P, Besso MJ, Sperling C, Kurth I, Baumann M, Brors B. Enhancing mass spectrometry imaging accessibility using convolutional autoencoders for deriving hypoxia-associated peptides from tumors. npj Syst Biol Appl. 2024;10:57.
- Eustace A, Mani N, Span PN, Irlam JJ, Taylor J, Betts GN, et al. A 26-gene hypoxia signature predicts benefit from hypoxia-modifying therapy in laryngeal cancer but not bladder cancer. Clin Cancer Res. 2013 Sep 1;19(17):4879-88.
- Grégoire V, Tao Y, Kaanders J, Machiels J, Vulquin N, Nuyts S, et al. Accelerated CH-RT with/without nimorazole for p16- HNSCC: The randomized DAHANCA 29-EORTC 1219 trial. Radiother. Oncol. 2021, 161, S187–S188
- Harris BH, Barberis A, West CM, Buffa FM. Gene Expression Signatures as Biomarkers of Tumour Hypoxia. Clin Oncol (R Coll Radiol). 2015 Oct;27(10):547-60.
- Janssen HL, Haustermans KM, Balm AJ, Begg AC. Hypoxia in head and neck cancer: how much, how important? Head Neck. 2005 Jul;27(7):622-38.
- Löck S, Perrin R, Seidlitz A, Bandurska-Luque A, Zschaeck S, Zöphel K, et al. Residual tumour hypoxia in head-and-neck cancer patients undergoing primary radiochemotherapy, final results of a prospective trial on repeat FMISO-PET imaging. Radiother Oncol. 2017 Sep;124(3):533-540.
- Machiels JP, René Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V; EHNS Executive Board. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020 Nov;31(11):1462-1475.
- Singleton DC, Macann A, Wilson WR. Therapeutic targeting of the hypoxic tumour microenvironment. Nat Rev Clin Oncol. 2021;18:751–772.
- Thomson DJ, Slevin NJ, Baines H, Betts G, Bolton S, Evans M, et al.; NIMRAD Trial Group. Randomized Phase 3 Trial of the Hypoxia Modifier Nimorazole Added to Radiation Therapy With Benefit Assessed in Hypoxic Head and Neck Cancers Determined Using a Gene Signature (NIMRAD). Int J Radiat Oncol Biol Phys. 2023 Dec 9:S0360-3016(23)08184-1.
- Toustrup K, Sørensen BS, Nordsmark M, Busk M, Wiuf C, Alsner J, Overgaard J. Development of a hypoxia gene expression classifier with predictive impact for hypoxic modification of radiotherapy in head and neck cancer. Cancer Res. 2011 Sep 1;71(17):5923-31.
- Zschaeck S, Löck S, Hofheinz F, Zips D, Saksø Mortensen L, Zöphel K, et al. Individual patient data meta-analysis of FMISO and FAZA hypoxia PET scans from head and neck cancer patients undergoing definitive radio-chemotherapy. Radiother Oncol. 2020 Aug;149:189-196.
Follow the Topic
-
npj Systems Biology and Applications
An online Open Access journal dedicated to publishing the premier research that takes a systems-oriented approach and encourages studies that integrate, or aid the integration of, data, analyses and insight from molecules to organisms and broader systems.

Related Collections
With Collections, you can get published faster and increase your visibility.
Phenotypic Plasticity: A Systems Approach
Publishing Model: Open Access
Deadline: Jul 30, 2026
Systems mechanobiology
Publishing Model: Open Access
Deadline: Sep 28, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in