Why People with Alcohol Use Disorder Still Know How to Be Prosocial – and What That Tells Us About the Brain
Published in General & Internal Medicine and Behavioural Sciences & Psychology
Why do people with alcohol use disorder (AUD) often struggle in social situations? One common theory suggests that long-term alcohol use might dull the brain’s ability to connect actions with social rewards – in other words, the sense of satisfaction from helping others. Our team set out to test this idea using standardized tasks of social learning and decision-making, and what we found surprised us.
It’s well known that AUD is related to difficulties in relationships. People with AUD often report smaller social networks, more interpersonal conflicts, and less willingness to engage in prosocial behaviors. But what drives these changes? One popular explanation is that chronic alcohol use alters how the brain processes rewards – making social rewards feel less meaningful compared to, say, the anticipated effect of a drink. This shift could reduce “prosocial behavior,” such as cooperation and altruism.
To dig deeper, we focused on a specific process known as social reward learning – the ability to learn from outcomes that benefit others. Imagine choosing an action that rewards someone else and remembering to do it again. That’s prosocial learning in action. If this ability is impaired in people with AUD, it could explain why social interactions become strained.
How We Tested It
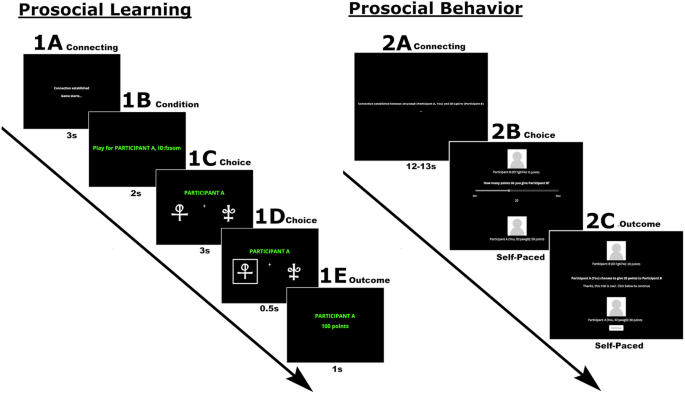
We ran two studies – one in the lab with Swedish participants, and one online with participants in the U.S. Over 470 young adults took part, about half of whom had moderate to severe AUD. In the main task, participants learned to choose symbols that rewarded either themselves, someone else, or no one at all (Figure 1A). In addition, we looked at their altruism in a game where they could give away points to a stranger (the “Dictator Game”, Figure 1B) and asked them to self-report how altruistic they tend to be in everyday life.
 and Behavior (B) In the first task assessing prosocial learning (A), participants repeatedly chose between two symbols. Each choice could lead to points being awarded in one of three conditions: • Self – “You get the points” • Other – “Another person gets the points” • No one – “No one gets the points” Over time, participants learned which symbol was more likely to give rewards. We used this setup to test whether people with alcohol use disorder (AUD) learn differently when rewards help someone else. In the second task assessing prosocial behavior (B), participants chose how many points they would like to give to another participant.")
Figure 1. How we measured Prosocial Learning (A) and Behavior (B)
In the first task assessing prosocial learning (A), participants repeatedly chose between two symbols. Each choice could lead to points being awarded in one of three conditions: Self – “You get the points”; Other – “Another person gets the points”; No one – “No one gets the points”
Over time, participants learned which symbol was more likely to give rewards. We used this setup to test whether people with alcohol use disorder (AUD) learn differently when rewards help someone else.
In the second task assessing prosocial behavior (B), participants chose how many points they would like to give to another participant.
Our Predictions – and the Unexpected Result
We expected that people with AUD would show reduced learning when the rewards were for someone else – a sign that they don’t learn from prosocial outcomes in the same way. But that didn’t happen. On average, both groups – those with and without AUD – performed similarly (Figure 2). They learned just as well when helping others as when helping themselves.
To make sure we weren’t missing effects on the underlying mechanistic level, we applied computational models that let us estimate the learning rate – a measure of how much someone updates their choices based on new experiences. Again, we found no meaningful differences between the AUD and control groups. Social learning and individual learning followed the same pattern in both groups. The brain’s machinery for learning from social rewards seems to remain intact in people with AUD.
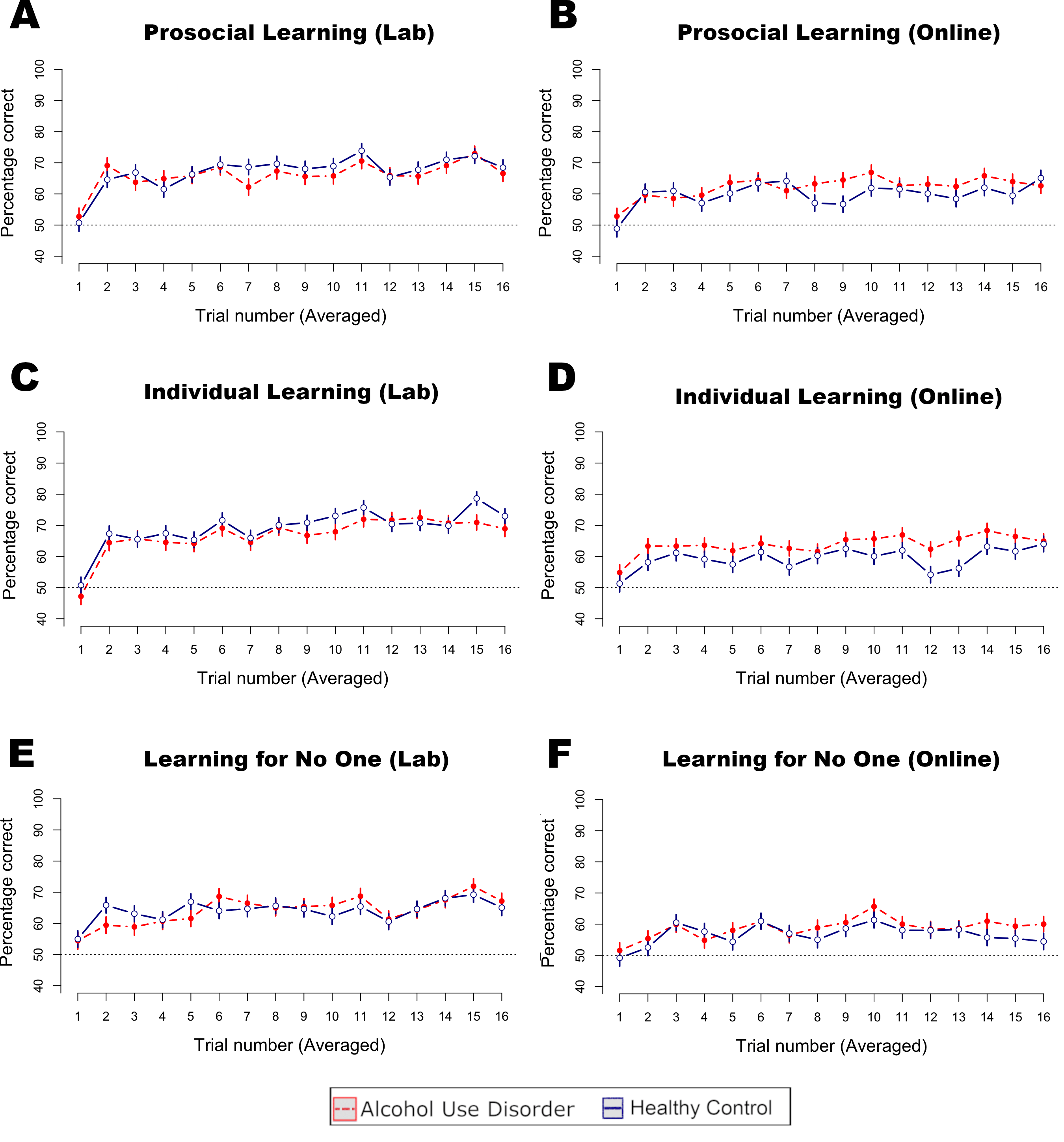
Figure 2. People with alcohol use disorder learned just as well as healthy individuals.
This graph shows how participants improved their choices over time in the learning task for the three conditions (prosocial learning (A and B); individual learning (C and D); and learning for no one (E and F). Higher lines mean better learning — choosing the symbol that gave more rewards.
Surprisingly, people with alcohol use disorder (AUD) learned just as well as those without AUD, whether the rewards went to themselves, to someone else, or to no one. This suggests that social learning itself is not impaired in AUD, even though prosocial behavior is reduced.
So Why Do They Help Less?
Interestingly, even though learning was preserved, people with AUD still showed reduced prosocial behavior. In both the Dictator Game and a self-report questionnaire, they demonstrated and reported reduced altruistic behavior. This mismatch tells us something important: social behavior and social learning might be driven by different brain processes. The problem isn’t that people with AUD can’t learn to help others – it may be that they choose not to, or value those actions less.
These findings challenge a common narrative that social deficits in AUD are rooted in basic learning problems. Instead, they point us toward other explanations – possibly involving social motivation and personality traits. For treatment, this opens new doors: rather than focusing solely on reward systems, interventions might need to boost social motivation or rebuild trust and relationships with others
As researchers, we were struck by how robust the social learning capacity was – even in individuals facing major challenges related to alcohol use. It reminds us that people with AUD still retain many cognitive strengths, which could be harnessed in recovery. And it underscores the importance of not making assumptions based on surface-level behavior.
Closing Thoughts
The brain’s reward systems are complex and resilient. Our work suggests that even when behavior seems impaired, the underlying learning processes may still be working fine. That’s a hopeful message – and a reminder to look deeper.
Follow the Topic
-
Translational Psychiatry
This journal focuses on papers that directly study psychiatric disorders and bring new discovery into clinical practice.

Related Collections
With Collections, you can get published faster and increase your visibility.
Moving towards mechanism, causality and novel therapeutic interventions in translational psychiatry: focus on the microbiome-gut-brain axis
Publishing Model: Open Access
Deadline: Nov 15, 2026
From mechanism to intervention: translational psychiatry of childhood maltreatment
Publishing Model: Open Access
Deadline: Sep 30, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in