
Duchenne muscular dystrophy (DMD) is a severe muscle-wasting disorder caused by the absence of functional dystrophin that affects 1 in 5000 males worldwide. The absence of functional dystrophin compromises muscle integrity, leading to progressive muscle wasting and weakness that causes mobility impairments and a shortened lifespan of 3 to 4 decades in patients with DMD. While there is no cure for DMD, the FDA recently approved restorative dystrophin gene therapy, however, it has only been approved for a subset of patients and, at best, can only partly increase dystrophin content. As a result, this therapy may only improve muscle health to a certain extent and essentially transform DMD into a milder disease known as Becker muscular dystrophy (BMD). Additionally, glucocorticoids are the gold standard treatment and most widely prescribed drugs for DMD and BMD as they improve muscle function in the short term, lower muscle inflammation, and delay the loss of ambulation by an average of 3 years. However, glucocorticoids are also associated with adverse metabolic effects such as insulin resistance, a heightened risk for type 2 diabetes, and osteoporosis, which can hasten disease outcomes and lead to early drug withdrawal. Therefore, alternative therapeutic options for patients with DMD should be explored.
Glycogen synthase kinase 3 (GSK3) is a well-known negative regulator of skeletal muscle mass and strength. The serine/threonine kinase has two isoforms, GSK3a and GSK3b, with the latter being the abundant and active isoform in muscle. It is a constitutively active enzyme, and its activity is regulated by phosphorylation, where Ser phosphorylation (Ser 21, GSK3a; and Ser9, GSK3b) inhibits GSK3 activity. We and others have shown that GSK3 can increase muscle mass, strength, regeneration, and the proportion of slow oxidative fibres in skeletal muscle, which altogether can help attenuate dystrophic pathology given that DMD is a condition where fast-twitch fibres are most affected. Additionally, previous studies have shown that GSK3 inhibition can alleviate other muscle wasting conditions such as myotonic dystrophy, limb-girdle muscular dystrophy, and muscle unloading. However, to our knowledge, there has been no study investigating whether inhibiting GSK3 can alleviate DMD pathology. Furthermore, GSK3 has been shown to be overactive in muscles obtained from the preclinical mdx mouse model for DMD – suggesting GSK3 as a plausible therapeutic target.
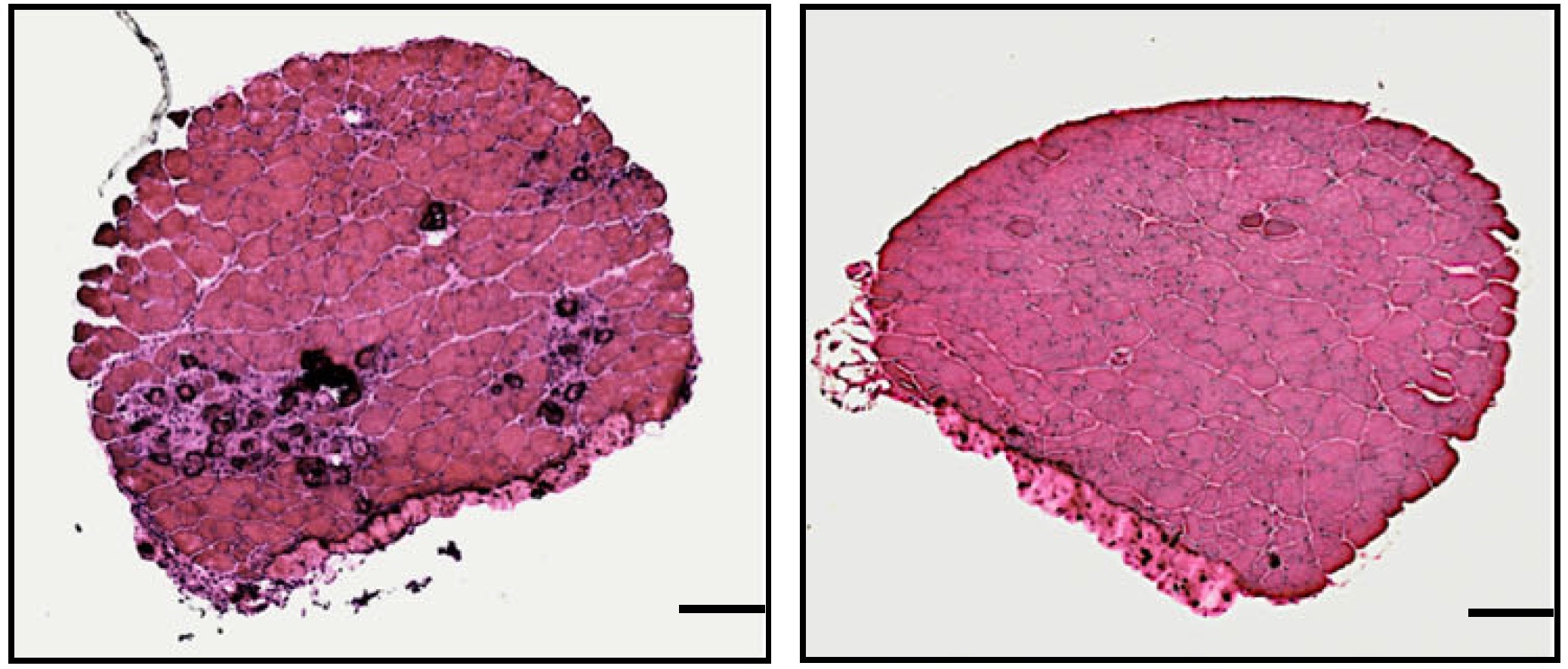
Using the severe DBA/2J (D2) and milder C57BL/10J (C57) male mdx mouse models of DMD, we demonstrated that inhibiting GSK3, pharmacologically or genetically and either alone or with exercise, improved skeletal muscle strength and endurance by promoting the oxidative fibre type and myogenesis. Additionally, these benefits come without any adverse effects on insulin signalling and bone health. In fact, GSK3 has been largely implicated in osteoporosis and type 2 diabetes, Thus, our study reveals GSK3 as a viable therapeutic target for the management of DMD.
Story behind GSK3 and DMD
The concept for this research was born from our lab’s interest in stimulating the oxidative fiber type through the enhancement of calcineurin signaling. Calcineurin is a calcium-dependent enzyme that, when activated, increases the expression of genes and, in turn, proteins that are typically found in oxidative fibres - one of these proteins being utrophin. Utrophin plays a similar role to dystrophin, and it can serve as a helpful substitute in conditions where dystrophin is absent, like DMD. With this in mind, activating calcineurin may combat DMD pathology and improve muscle health and performance! However, GSK3 tends to work against calcineurin signalling. Thus, the main idea behind this project was to stop GSK3 activity to enhance calcineurin signalling, to then increase the oxidative fiber type and with it, utrophin levels.
To do this, we used two drugs known to inhibit GSK3: lithium, which is already FDA-approved, and tideglusib, which is in clinical trials for another muscular dystrophy called myotonic dystrophy type 1. We felt that using these drugs was an advantage in that if they were successful in the pre-clinical realm, then our results might provide the push needed to move toward clinical trials for DMD. As the results rolled in, we began to see that inhibiting GSK3 in mdx mice offered even more advantages! Not only did it promote the oxidative fiber type and utrophin content, but it also increased muscle size and strength, and enhanced muscle repair. Additionally, these benefits to muscle health and performance came without any adverse effects to bone health or insulin sensitivity.
These promising results helped secure a partnership with AMO-Pharma that produces and distributes the GSK3 inhibitor, tideglusib. With their support in providing us additional tideglusib, we conducted more experiments in slightly older D2 mdx mice, as well as on mdx mice of the traditional C57 strain – all of which showed benefits to muscle strength and/or endurance. To truly highlight the benefits of stopping GSK3 for muscle health in DMD, we genetically modified the mdx mice in a way that reduced their GSK3 protein by about 40%, specifically in their skeletal muscles. We call this approach a knockdown, and by knocking down GSK3 in the muscles from mdx mice, we saw signs of attenuated muscular dystrophy and an improvement in both muscle strength and endurance.
Finally, before the acceptance of our manuscript, we realised that it would be beneficial if we could somehow study GSK3 in muscle cells obtained from patients living with DMD. Thanks to our collaborator, Dr. Gabsang Lee, we received muscle cells from two patients living with DMD. Our experiments showed that the GSK3 levels in these muscle cells were virtually the same as in the healthy control cells. However, we did notice some signs that could suggest GSK3 may still be overactive. Essentially, when GSK3 is overactive, it leads to a decrease in a protein known as beta-catenin. We observed that DMD muscle cells contained only small amounts of this essential protein compared to healthy muscle cells. This finding is particularly significant for DMD because beta-catenin plays a vital role in a pathway that encourages muscle repair and regeneration – both of which are crucial for DMD patients. Additionally, we and others have previously shown that stopping GSK3 in otherwise healthy muscle cells can raise the levels of beta-catenin to promote the development of muscle, which altogether suggests that GSK3 may be a viable target for DMD.
Look Ahead
Our study is the first to demonstrate the therapeutic potential of GSK3 inhibition for DMD, with its inhibition possibly improving many aspects of muscle and metabolic health. We look forward to testing whether targeting GSK3 can be used for longer periods of time or whether it can be combined with current (i.e., glucocorticoid) or emerging (gene therapy) treatments for DMD. We will also conduct experiments testing whether stopping GSK3 in human DMD muscle cells can restore the muscle developmental process by raising beta-catenin. Collectively, these experiments may forge a pathway to the clinical setting, aiming to positively impact those affected by DMD.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Tumor Microenvironment Crosstalk and Therapeutic Implications
Publishing Model: Hybrid
Deadline: Nov 02, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in